Prevalence of Hepatitis B Virus Infection Among Some Residents of Wukari Metropolis, Nigeria
-
Chinedu Imo


Department of Biochemistry, Faculty of Pure and Applied Sciences, Federal University Wukari, Wukari, Nigeria
Anagu EzekielWukari Study Centre, Department of Public Health, Faculty of Health Sciences, National Open University of Nigeria, Abuja, Nigeria
| Received 28 Oct, 2024 |
Accepted 29 Nov, 2024 |
Published 31 Mar, 2025 |
Background and Objective: Hepatitis B is a contagious disease that affects the liver, caused by Hepatitis B Virus (HBV). It poses a significant health risk to many people, as it can result in chronic infection and individuals affected can be at a high risk of death from liver cancer or cirrhosis. This study investigated the prevalence of hepatitis B virus infection among some Wukari Metropolis, Nigeria residents. Materials and Methods: This investigative research study used 60 adult residents of Wukari Metropolis, Taraba State, Nigeria comprising 30 males and 30 females. The selected individuals who volunteered were all adults. Detection of Hepatitis B Surface Antigen (HBsAg) was carried out on the individuals using a rapid diagnostic HBsAg test strip. Results: The result of the study showed there was a negative test result for HBsAg in 26 males and 27 females, while there was a positive test result for HBsAg in 4 males and 3 females among the volunteered residents of Wukari Metropolis, Taraba State, Nigeria. Seven out of the 60 residents of Wukari Metropolis evaluated tested positive for HBsAg, while 53 residents tested negative for HBsAg. About 13.33% of male residents tested had HBV infection, while 10% of the female residents tested had HBV infection. About 11.67% of the total population tested had HBV infection. Conclusion: This study concluded that the prevalence of hepatitis B virus infection among Wukari Metropolis, Nigeria residents could be about 11.67%.
| Copyright © 2025 Imo and Ezekiel. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
An inflammation of the liver tissue is a symptom of hepatitis. While some hepatitis patients or animals may show no symptoms at all, others may have jaundice or yellow discoloration of the skin and whites of the eyes, as well as poor appetite, nausea, vomiting, fatigue, abdominal pain and diarrhea. If hepatitis goes away in six months, it is considered acute; if it lasts longer than six months, it is considered chronic. According to Bernal and Wendon1, acute hepatitis can either go away on its own, develop into chronic hepatitis or (very infrequently) result in abrupt liver failure. Cancer, liver failure and cirrhosis can develop from chronic hepatitis.
For thousands of years, people have struggled with viral hepatitis. Hippocrates reported similar occurrences of jaundice on the Island of Thasos in the fifth century BC and epidemics have been recorded in China as early as 5000 years ago2. Immunization helps prevent hepatitis A, B and D. Drugs can be used to treat chronic viral hepatitis. All people with chronic hepatitis C should take antiviral drugs, except those who have health issues that shorten their life expectancy3.
The symptoms of hepatitis can vary greatly, ranging from severe liver failure to no symptoms at all. A viral infection is typically the source of the acute form of hepatitis, which manifests as broad symptoms that typically go away on their own. Although chronic hepatitis might manifest similarly, it can also exhibit particular liver dysfunction symptoms brought on by chronic inflammation and injury to the liver4.
The most common kind of hepatitis worldwide, especially in Asia and Africa, is viral hepatitis. Hepatitis A, B, C, D and E are the five viruses that cause it. Both hepatitis A and E are self-limiting diseases that do not progress to chronic hepatitis, are more prevalent in underdeveloped nations and are spread by the fecal-oral route5. Exposure to contaminated blood and bodily fluids, including semen and vaginal secretions, can spread the illnesses hepatitis B, C and D. While hepatitis D only occurs in those who have hepatitis B co-infection and requires hepatitis B to replicate, hepatitis B and C can cause acute or chronic infections5.
Depending on the underlying cause, hepatitis can harm the liver in different ways. Usually, the liver sustains damage first, which sets off an inflammatory reaction that may eventually become chronic. Cirrhosis and increasing fibrosis may result from this5. The precise mechanism is better understood in the case of viral hepatitis brought on by hepatitis B or C. Instead of directly killing cells, the viruses infect liver cells, which sets off an immunological reaction that damages the cells and causes inflammation. Activating the death receptor-mediated signaling pathway may cause viral-induced apoptosis5,6. The infection can either be eradicated (acute disease) or continue (chronic disease), depending on the immune response’s intensity, the immune cells’ kinds and the virus’s capacity to elude the body’s defenses. The virus causes repeated cycles of inflammation, damage and wound repair when it persists in liver cells. This eventually results in fibrosis or scarring and hepatocellular cancer. Chronic infections are more likely to occur in those with compromised immune systems. Natural killer cells, which produce a cytokine milieu that attracts CD4 T-helper and CD8 cytotoxic T-cells, are the main forces behind the early innate response7,8. Type I interferons are the cytokines that drive the antiviral response7.
A patient’s medical history, symptoms, blood tests, imaging and occasionally a liver biopsy are all taken into consideration while making a hepatitis diagnosis. For the diagnosis of viral and other acute causes of hepatitis, blood testing and clinical presentation are typically enough. Nonetheless, a liver biopsy is regarded as the gold standard for diagnosis in chronic instances where blood testing might not be helpful. Because a biopsy is invasive and has a slight risk of bleeding, which is increased in patients with cirrhosis and liver damage, it is typically not the first diagnostic procedure9. The degree and pattern of inflammation and fibrosis can be precisely determined by histopathologic examination if a biopsy is carried out10. To stop the disease from spreading, it is crucial to follow general measures. Except for those with hepatitis B and C who have uncontrollable bleeding and those with hepatitis A and E who have faecal incontinence, isolation is usually not necessary5.
Several people worldwide, particularly in Wukari, Taraba State, Nigeria, are afflicted with hepatitis B. Long-term health issues such as liver damage, liver failure, liver cancer and even death can arise from untreated chronic hepatitis B. The illness has a significant financial impact on both people and governments. Costs for individuals and their families include getting medications to treat the illness at home, traveling to clinics and dispensaries, missing work or school, paying for preventative care and paying for funerals in the event of a death. The costs of maintaining, stocking and staffing medical institutions, buying medications and supplies and putting public health initiatives against the illness into action, on the other hand, fall on governments.
It is believed that the prevalence rate of hepatitis B is increasing and the lack of awareness campaigns against hepatitis B is becoming a major challenge. This has led to a rise in hepatitis B cases, making it a growing public health concern. Many individuals who are infected with the hepatitis B virus remain unaware of their condition due to limited testing and awareness campaigns surrounding the disease. This study investigated the prevalence of Hepatitis B Virus (HBV) infection within a specific population, analyzing the rate of infection, associated risk factors and any demographic or behavioral variables that might contribute to its spread.
MATERIALS AND METHODS
Study area and duration: This project research study was carried out from March to April, 2024 in the Wukari Metropolis, Taraba State, Nigeria.
Study population ethical consent: Sixty adult residents of the Wukari Metropolis in Taraba State, Nigeria, comprising of 30 males and 30 females, volunteered and were used for this research study. All participants were 18 years and above and gave their consent for the testing.
Materials and equipment used: The following materials and equipment were used during the present study: Rapid diagnostic HBsAg test strip (product of Nantong Egens Biotechnology Co., Ltd. China), syringe, blood specimen, specimen collection container, sterile wipe, disposable plastic pipette, timer, cotton wool and centrifuge.
Principles of rapid diagnostic HBsAg test strip for detection of HBsAg: The hepatitis B surface antigen test (serum/plasma) is a lateral flow chromatographic immunoassay based on the principle of the double antibody-sandwich technique. The membrane is pre-coated with anti-HBs on the test line region of the test. While detecting a positive sample, HBsAg in the specimen (serum or plasma) reacts with the particle coated with anti-HBs. The mixture migrates upward on the membrane chromatographically by capillary action to react with the anti-HBs on the membrane and generate a colored line. The presence of this colored line in the test region indicates a positive result, while its absence indicates a negative result. To serve as a procedural control, a colored line will always appear in the control line region indicating that the proper volume of specimen has been added and membrane wicking has occurred.
Procedure for detection of HBsAg: A blood sample was collected from each of the volunteers by vein puncture. The blood sample was dispensed into a clean labeled specimen collection tube (containing no anticoagulant) and allowed to stand for 10 min to clot before being centrifuged at 3000 rpm for 10 min. The serum was separated from the clot using a pipette and dispensed into a new clean labeled sample tube.
A pouch of the rapid test strip was opened at the notch and the test device was removed. The device (strip) was labeled with the volunteer’s ID number. The strip was immersed into the serum with the arrow end pointing towards the serum. The strip was taken out of the serum after 10 sec and laid flat on a clean, dry and flat surface. The timer was set up immediately and the result on the test strip was read and interpreted within 15 min.
RESULTS AND DISCUSSION
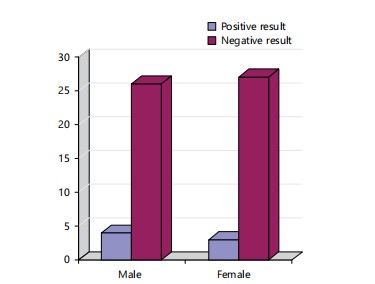
Positive result: In addition to a pink-colored control (C) band, a distinct pink-colored band also appeared in the test (T) region; Negative result: Only one colored band appeared on the control (C) region. No apparent band on the test (T) region; Invalid result: No visible colored band in the control region or a colored band observed only in the test region. Therefore, results of the study are presented in Fig. 1 and Table 1.
|
| Table 1: | Detection of HBsAg in some residents of Wukari Metropolis, Nigeria | |||
| Sex | Number of HbsAg positive test result |
Number of HbsAg negative test result |
Total number of test results |
Positive test results (%) |
Remark |
| Male | 4 | 26 | 30 | 13.33 | Four cases of HBV infection |
| Female | 3 | 27 | 30 | 10 | Three cases of HBV infection |
| Both male and female | 7 | 53 | 60 | 11.67 | Seven cases of HBV infection |
Figure 1 showed that there was a negative test result for HBsAg in 26 males and 27 females, while there was a positive test result for HBsAg in 4 males and 3 females among the volunteered residents of Wukari Metropolis, Taraba State, Nigeria.
Table 1 shows that 7 out of the 60 residents of the Wukari Metropolis tested positive for HBsAg, while 53 residents tested negative for HbsAg. About 13.33% of male residents tested had HBV infection, while 10% of the female residents tested had HBV infection. About 11.67% of the total population tested had HBV infection.
Detecting the presence of hepatitis B surface antigen is an important method for diagnosing hepatitis B virus infection. This study conducted in Wukari Metropolis; Nigeria revealed the possible prevalence of hepatitis B virus infection among its residents. A positive test result during diagnosis is usually an indication of hepatitis B virus infection, which can cause both acute and chronic infections. Some individuals can be infected with hepatitis B without experiencing any symptoms until they are tested. This is because hepatitis B infection can be asymptomatic and easily go unnoticed11,12.
The result of this study showed that there was a negative test result for HBsAg in 26 males and 27 females, while there was a positive test result for HBsAg in 4 males and 3 females among the volunteered residents of Wukari Metropolis, Taraba State, Nigeria (Fig. 1). This suggests that more males may be infected with the hepatitis B virus than females residing in the Wukari Metropolis, which implies that more males may be suffering from hepatitis B than females among those residing in the Wukari Metropolis. Those who tested positive may experience some ill-health concerns such as liver-related problems if not treated. This is because chronic hepatitis has been reported by Dienstag et al.4 to present similarly, but can manifest signs and symptoms specific to liver dysfunction with long-standing inflammation and damage to the organ. Based on the result of this study, more males may be prone to hepatitis B due to many factors that expose them to the risk factors of hepatitis B more than females. The lifestyle of the male folks may also contribute to the reasons for this increased prevalence of hepatitis B among males than the female folks.
It is believed that male folks get involved in more activities that may require body contact than females. It is also believed that most men usually get involved with multiple sex partners than most women, which may contribute to the rate of exposure to the hepatitis B virus. The findings of this study showed that about 86.67% of the adult male and 90% of the adult female residents of the Wukari Metropolis are free from the hepatitis B virus and as such, may not be suffering from hepatitis B. Testing for hepatitis B infection is recommended because anybody can be infected by hepatitis B virus. Even the healthcare staff are also at an increased risk of infection13.
This study result suggests that about 13.33% of the males residing in the Wukari Metropolis may be infected with the hepatitis B virus and as such may be suffering from hepatitis B. On the other hand, the result also suggested that about 10% of the females residing in the Wukari Metropolis may be infected with the hepatitis B virus and as such may be suffering from hepatitis B. This shows that there is a need to engage in awareness programs regarding the prevention and treatment of hepatitis B among people residing in different parts of Nigeria, especially, the Wukari Metropolis. It is also possible that the reason for the current prevalent rate of hepatitis B among the males and the females residing in the Wukari Metropolis may be due to the current level of awareness. Health workers and the government are hereby encouraged to intensify the level of awareness campaigns and management strategies towards tackling the occurrence of hepatitis B among citizens. If hepatitis B is not treated, it may become a predisposing factor for hepatitis D. This is because hepatitis D has been reported to be a defective virus infection that requires hepatitis B to replicate and is only found with hepatitis B co-infection5. According to Gan et al.14, there is a link between hepatitis B and membranous glomerulonephritis as well as other health conditions.
Among the total population tested in this study, 7 out of the 60 volunteers tested positive for HBsAg which implies that 7 out of 60 residents of Wukari Metropolis may be infected with hepatitis B virus. This result suggested that about 11.67% of the adults residing in the Wukari Metropolis may be suffering from hepatitis B, while about 88.33% of the adults residing in Wukari Metropolis may be free from hepatitis B. This finding showed that more people among the adults residing in Wukari Metropolis may be safe from hepatitis B than those who may be infected with the hepatitis B virus. Creating more awareness of hepatitis B virus infection and hepatitis B among residents of Wukari may contribute in reducing this prevalence rate. The more people know about the various ways to avoid hepatitis B virus infection, the more likely they are to stay free of hepatitis B. According to a report by Pungpapong et al.15, hepatitis B infection has been preventable since 1982 through vaccination. The World Health Organization (WHO) also recommends that infants receive the vaccine within 24 hrs of birth, where possible12.
This study revealed that the prevalence rate of hepatitis B virus infection among adult residents of the Wukari Metropolis is 11.67%. The prevalence rate of hepatitis B among various cities is expected to contribute to the regional prevalence. It was previously reported that in 2021, 19 African countries had infection rates ranging between 8-19%, placing them in the high prevalence category16. According to the findings of this current study, the government and healthcare workers should improve vaccination for individuals who are not affected by the hepatitis B virus and provide treatment for those who tested positive for hepatitis B surface antigen. By doing this, the number of people with hepatitis B in the Wukari Metropolis can be significantly reduced, if not eliminated. This study supports the findings of a previous study of Castaneda et al.17, which suggested that primary care physicians and gastroenterologists need to have a comprehensive understanding of hepatitis to provide proper care to patients.
CONCLUSION
This study showed that about 13.33% of male residents of Wukari Metropolis, Nigeria tested had HBV infection, while 10% of the female residents tested had HBV infection. More male residents of the Wukari Metropolis are infected with the hepatitis B virus than female residents. Seven out of the 60 residents of Wukari Metropolis evaluated tested positive for HBsAg, while 53 residents tested negative for HBsAg. About 11.67% of adults residing in the Wukari Metropolis may have HBV infection. There is need for regular testing of individuals living in both urban and rural areas of different part of Nigeria to ascertain the prevalence of HBV infection. There is need to increase the campaign for the awareness of HBV infection in every part of Nigeria.
SIGNIFICANCE STATEMENT
This lack of diagnosis can lead to severe health consequences and even death. Therefore, there is a pressing need for research into this current study. This study holds great importance as it aims to investigate the prevalence of hepatitis B virus infection among individuals residing in the Wukari Metropolis, Nigeria. The findings of this research will reveal the rate of occurrence of hepatitis B virus infection among residents of the Wukari Metropolis in Taraba State, Nigeria.
REFERENCES
- Bernal, W. and J. Wendon, 2013. Acute liver failure. N. Engl. J. Med., 369: 2525-2534.
- da Fonseca J.C.F., 2010. History of viral hepatitis. Rev. Sociedade Bras. Med. Trop., 43: 322-330.
- AASLD/IDSA HCV Guidance Panel, 2015. Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology, 62: 932-954.
- Dienstag, J.L., 2022. Chronic Hepatitis. In: Harrison's Principles of Internal Medicine, 21e, Loscalzo, J., A. Fauci, D. Kasper, S. Hauser, D. Longo and J.L. Jameson (Eds.), McGraw-Hill Education, New York,.
- Llaneras, J., M. Riveiro-Barciela, A. Rando-Segura, C. Marcos-Fosch and L. Roade et al., 2020. Etiologies and features of acute viral hepatitis in Spain. Clin. Gastroenterol. Hepatol., 19: 1030-1037.
- Nakamoto, Y. and S. Kaneko, 2003. Mechanisms of viral hepatitis induced liver injury. Curr. Mol. Med., 3: 537-544.
- Heim, M.H. and R. Thimme, 2014. Innate and adaptive immune responses in HCV infections. J. Hepatol., 61: S14-S25.
- Rehermann, B., 2015. Natural killer cells in viral hepatitis. Cell. Mol. Gastroenterol. Hepatol., 1: 578-588.
- Grant, A. and J. Neuberger, 1999. Guidelines on the use of liver biopsy in clinical practice. Gut, 45: IV1-IV11.
- Sharma, I. and D. Choudhury, 2015. Histopathological patterns of gall bladder diseases with special reference to incidental cases: A hospital based study. Int. J. Res. Med. Sci., 3: 3553-3557.
- Terrault, N., B. Roche and D. Samuel, 2005. Management of the hepatitis B virus in the liver transplantation setting: A European and an American perspective. Liver Transplant., 11: 716-732.
- Downs, L.O., K. Kabagambe, S. Williams, E. Waddilove and M. Delphin et al., 2024. Peer support for people living with hepatitis B virus-A foundation for treatment expansion. J. Viral Hepatitis, 31: 490-499.
- Garthwaite, E., V. Reddy, S. Douthwaite, S. Lines, K. Tyerman and J. Eccles, 2019. Clinical practice guideline management of blood borne viruses within the haemodialysis unit. BMC Nephrol., 20.
- Gan, S.I., S.M. Devlin, N.W. Scott-Douglas and K.W. Burak, 2005. Lamivudine for the treatment of membranous glomerulopathy secondary to chronic hepatitis B infection. Can. J. Gastroenterol. Hepatol., 19: 625-629.
- Pungpapong, S., W.R. Kim and J.J. Poterucha, 2007. Natural history of hepatitis B virus infection: An update for clinicians. Mayo Clinician Proc., 82: 967-975.
- Cruz, H.M., V.S. de Paula and L.M. Villar, 2008. A cross-sectional study of viral hepatitis perception among residents from Southeast and Sorth regions of Brazil. Int. J. Environ. Res. Public Health, 15.
- Castaneda, D., A.J. Gonzalez, M. Alomari, K. Tandon and X.B. Zervos, 2021. From hepatitis A to E: A critical review of viral hepatitis. World J. Gastroenterol., 27: 1691-1715.
How to Cite this paper?
APA-7 Style
Imo,
C., Ezekiel,
A. (2025). Prevalence of Hepatitis B Virus Infection Among Some Residents of Wukari Metropolis, Nigeria. Asian Journal of Biological Sciences, 18(1), 146-151. https://doi.org/10.3923/ajbs.2025.146.151
ACS Style
Imo,
C.; Ezekiel,
A. Prevalence of Hepatitis B Virus Infection Among Some Residents of Wukari Metropolis, Nigeria. Asian J. Biol. Sci 2025, 18, 146-151. https://doi.org/10.3923/ajbs.2025.146.151
AMA Style
Imo
C, Ezekiel
A. Prevalence of Hepatitis B Virus Infection Among Some Residents of Wukari Metropolis, Nigeria. Asian Journal of Biological Sciences. 2025; 18(1): 146-151. https://doi.org/10.3923/ajbs.2025.146.151
Chicago/Turabian Style
Imo, Chinedu, and Anagu Ezekiel.
2025. "Prevalence of Hepatitis B Virus Infection Among Some Residents of Wukari Metropolis, Nigeria" Asian Journal of Biological Sciences 18, no. 1: 146-151. https://doi.org/10.3923/ajbs.2025.146.151

This work is licensed under a Creative Commons Attribution 4.0 International License.