Demographic Characteristics and ABO Blood Group Genotype Distribution among Sickle Cell Anaemia Patients in Lagos, Southwest Nigeria
-
Yahaya Tajudeen


Department of Biological Sciences, Federal University Birnin Kebbi, Kebbi State, Nigeria
Adewale Mutiyat KehindeDepartment of Biological Sciences, Federal University Birnin Kebbi, Kebbi State, Nigeria
Olamide OkeDepartment of Biology, National Open University of Nigeria, Lagos
Moronkeji AkinpeluDepartment of Medical Laboratory Science, University of Medical Sciences, Ondo, Ondo State, Nigeria
Danjuma Jamilu KokoDepartment of Biological Sciences, Federal University Birnin Kebbi, Kebbi State, Nigeria
Usman Bello MuhammadDepartment of Biological Sciences, Federal University Birnin Kebbi, Kebbi State, Nigeria
| Received 14 Nov, 2024 |
Accepted 03 Dec, 2024 |
Published 31 Mar, 2025 |
Background and Objective: Research emphasizes the significance of demographic data and ABO blood group genotypes in the effective management of sickle cell anemia. Unfortunately, there is a lack of such information for sickle cell anemia patients in Lagos, Nigeria. This study aimed to determine the demographic characteristics, ABO blood group genotypes and sickle cell genotypes of patients with sickle cell anemia in Lagos, Nigeria. Materials and Methods: Data were collected using a structured checklist from the medical records of 170 sickle cell anemia patients who attended selected medical facilities in the city between January, 2024 and August, 2024. Results: The results revealed a predominance of patients aged 40 years and above (28.82%), followed by those in the 11-20 and 21-30 age groups (20.00% each). The male-to-female ratio was approximately 1:1. The O+ blood group genotype was the most common (24.71%), followed by A+ (23.53%), while AB‾ was the least prevalent (1.77%). Regarding disease severity, blood group O+ had the fewest severe cases, with 16 (38.10%) patients, while all patients with AB+ and AB‾ blood groups exhibited severe forms of the disease. The HbSS was the dominant sickle cell genotype, present in 90.14% of the patients. Conclusion: Based on these findings, efforts should be made to ensure an ample supply of O+ and A+ blood types in blood banks. Non O‾ blood groups should receive special attention, as they are associated with more severe forms of the disease. Medical practitioners should consider individual blood groups when planning treatment.
| Copyright © 2025 Tajudeen et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Sickle cell anemia is a genetic disorder characterized by the deformation of red blood cells, causing them to break down prematurely1. The condition arises due to a single mutation in the β-globin gene on chromosome 11. At the 17th nucleotide, adenine replaces thymine, altering the genetic sequence. This mutation follows an autosomal recessive inheritance pattern. Individuals may inherit one altered gene (heterozygous AS) or two mutated copies (homozygous SS) from their parents. Individuals with one normal allele and one mutated allele are carriers (sickle cell trait) and generally do not exhibit severe symptoms2-4. Individuals with homozygous SS produce abnormal Hemoglobin S (HbS), which can cause red blood cells to become stiff and adopt the characteristic sickle shape under certain conditions, such as low oxygen levels or dehydration3. Due to their lack of flexibility, sickle cells die early and often become lodged in small blood vessels, blocking the flow of oxygen-rich blood to tissues and organs, leading to serious health problems throughout the body5. These health issues include acute pain, fatigue, jaundice, tissue and organ damage, priapism, delayed growth, increased risk of infections, pneumonia and acute chest syndrome, stroke and kidney, liver and heart disease6,7.
Sickle cell anemia substantially induces multi-morbidity and impairs quality of life while straining healthcare systems wherever it exists8,9. The global incidence of the disease is on the rise. Between 2000 and 2021, the number of people living with sickle cell disease globally increased by 41.4%, from 5.46 million in 2000 to 7.74 million in 202110. During this period, the mortality burden of sickle cell disease was nearly 11 times higher 10. In the United States, sickle cell disease affects about 100,000 people annually, of whom over 90% are non-Hispanic Black or African American and an estimated 3-9% are Hispanic or Latino11. In Africa, due to delayed diagnosis and/or lack of access to comprehensive care, early childhood (under 5 years) mortality is high, with approximately 500 children with sickle cell disease dying prematurely every day on the continent12. Nigeria has the highest burden of sickle cell disease globally, with approximately 1 in 4 Nigerians carrying the sickle cell mutation13. About 20% of children aged 6-59 months are affected by the condition13. The prevalence of sickle cell disease in Nigeria is influencing societal norms, including dating, marriage and life planning, reflecting the profound impact of the disease on the country’s population. The economic burden of managing sickle cell disease is also high. According to Baldwin et al.14, costs are higher for sickle cell disease patients compared to non-sickle cell individuals, with a cost difference ranging from 6,636-63,436$ annually. Parents of sickle cell patients also undergo significant psychosocial burden and stress15.
Currently, there is no known cure for sickle cell anemia, but effective management strategies and treatments can help reduce the frequency and severity of pain episodes, improving the quality of life for those affected1. The severity of sickle cell disease arises from various clinical complications that impact each individual’s immunity. Therefore, preventive and management strategies tailored to individuals or populations are likely to be more effective16. The ABO blood group genotypes, along with demographic factors such as gender, age and marital status, play a significant role in influencing disease prevalence and treatment outcomes, as highlighted in various studies. These factors should be considered when developing preventive and management strategies. Specifically, these factors have been shown to affect the prevalence and management of sickle cell anemia in Birnin Kebbi, Nigeria1 and in Umuahia, Abia State, Nigeria11. In Lagos, Nigeria, there is a lack of comprehensive research on the incidence, demographic factors and blood group genotype associations related to sickle cell anemia, highlighting the need for this investigation. Therefore, this study is urgently needed to address this critical issue. The main aim of this study was to analyze the distribution of ABO blood group genotypes, sickle cell genotypes and demographic features among individuals with sickle cell anemia in Lagos, Nigeria.
MATERIALS AND METHODS
Study population and data collection: A retrospective random sampling of sickle cell disease patients who attended selected medical facilities in Lagos between January and August, 2024 was conducted. Relevant medical information about the patients was collected using a standardized checklist, which comprised two sections: Section I and Section II. Section I covered socio-demographic variables, including the patient's age, gender and ethnicity. Section II focused on medical information, specifically the ABO blood group genotypes, sickle cell genotypes and the severity of sickle cell anemia. All data were analyzed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, New York, USA). This study received approval from the Ethics Committee of the National Open University of Nigeria, Lagos (approval number: NOUN/25/2024) on 25 January, 2024.
Scoring of the severity of the disease: The severity of the disease was evaluated based on the frequency of hospital visits or the number of episodes per month. The classification was done according to ABO blood group genotypes. Conditions with three visits per month were classified as very severe, two visits as severe, one visit per month as moderately severe and one visit every two months as mild.
Determination of sample size: The sample size was calculated using Equation 117.
| (1) |
where, N is the number of individuals with sickle cell disease who attended the hospitals between January and August, 2024 and e is the level of precision, typically between 0.10 and 0.01 (i.e., 10 to 1%).
Using a level of precision (e) of 5% and a population size (n) of 294:
where, n = 169.5, resulting in ~170.
Rounding up, the sample size used was 170.
Validation of tool: Statistical validation was systematically performed on each question to assess construct validity. A manual validation process was also conducted for physical records and a questionnaire was distributed to patients. The questionnaire was meticulously designed to effectively determine individual patients' disease status. These methodological approaches collectively contribute to a robust assessment of validity.
Eligibility criteria: The inclusion criteria comprised eligible medical records of all patients diagnosed with sickle cell anemia between January and August, 2024. Exclusion criteria included individuals outside the specified duration, those with incomplete records and patients not diagnosed with sickle cell anemia.
RESULTS
Demographic data of sickle cell disease patients: Table 1 shows the age, gender and ethnic of sickle cell disease patients in Lagos, Nigeria. The highest proportion (28.82%) were 40 years or older, followed by equal proportions in the 11-20 and 21-30-year age ranges (20.00% each). Smaller proportions were observed in the 1-10 and 31-40 year age ranges, accounting for 16.47 and 14.71%, respectively. The results revealed a slight female predominance, with females accounting for 52.94% (n = 90) of the total population, while males accounted for 47.06% (n=80). The Yoruba ethnic group accounted for the majority, with 87 patients (51.18%), followed by the Igbo with 50 patients (29.40%). The Edo had 16 patients (9.41%), the Hausa 8 patients (4.71%), the Efik 7 patients (4.12%) and the Ijaw 2 patients (1.18%).
ABO blood groups genotypes of the patients: Table 2 shows the ABO blood groups of the sickle cell anemia patients. Blood group O+ had the highest number of patients with 42 (24.71%), followed by blood group A+ with 40 (23.53%), blood group B+ with 27 (15.88%), blood group B– with 21 (12.35%), blood group O– with 12 (7.06%), blood group AB+ with 5 (2.94%) and blood group AB– with 3 (1.77%) patients.
|
| Table 1: | Demographic characteristics of sickle cell disease patients | |||
| Variables | Age | Frequency n (%) |
| Age | 01-Oct | 28 (-16.47) |
| Nov-20 | 34 (-20) | |
| 21-30 | 34 (-20) | |
| 31-40 | 25 (-14.71) | |
| 41-50 | 49 (-28.82) | |
| Total | 170 (-100%) | |
| Gender | Male | 80 (-47.06) |
| Female | 90 (-52.94) | |
| Total | 170 (-100%) | |
| Ethnic | Yoruba | 87 (-51.18) |
| Igbo | 50 (-29.4) | |
| Edo | 16 (-9.41) | |
| Hausa | 8 (-4.71) | |
| Efik | 7 (-4.12) | |
| Ijaw | 2 (-1.18) | |
| Total | 170 (-100%) |
| Table 2: | Distribution of ABO blood group genotypes among the sickle cell disease patients | |||
| Blood group | Frequency n (%) | Severe cases n (%) |
| A+ | 40 (23.53) | 25 (62.50) |
| A– | 20 (11.76) | 10 (50.00) |
| B+ | 27 (15.88) | 22 (81.48) |
| B– | 21 (12.35) | 16 (76.19) |
| AB+ | 5 (2.94) | 5 (100) |
| AB– | 3 (1.77) | 3 (100) |
| O+ | 42 (24.71) | 16 (38.10) |
| O– | 12 (7.06) | 11 (91.7) |
Regarding disease severity, blood group O+ had the least severe cases, with 16 (38.10%) patients, while all AB+ and AB– blood groups expressed severe form of the disease.
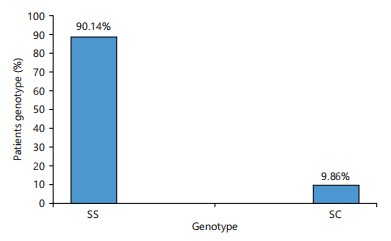
Genotypes of the sickle cell patients: Figure 1 shows the distribution of sickle cell disease genotypes among the patients. The majority, 90.14%, have the more severe form of sickle cell disease (HbSS), while 9.86% have the milder form (HbSC).
DISCUSSION
This study determined the distribution of demographic characteristics, ABO blood group genotypes and sickle cell genotypes among sickle cell anemia patients in Lagos, Nigeria. Analysis of retrospective demographic data from hospital records showed that females were disproportionately affected by sickle
cell anemia, with a higher frequency of cases compared to males. These findings are consistent with those of Yahaya et al.1, Nwabuko et al.11 and Oluwadamilola et al.18, who all reported a higher occurrence of sickle cell anemia among females than males in Birnin Kebbi, Kebbi State, Nigeria; Umuahia, Abia State, Nigeria and Osogbo, Osun State, Nigeria, respectively. However, the results contradict those of Adigwe19 among unmarried adults in Abuja, Nigeria and Ugwu20 in Enugu, Nigeria. The demographic data further showed that sickle cell anemia was most prevalent among adults aged 40 years and older. This finding aligns with the results of Seck et al.21 in Senegal. A systematic review by Thein et al.22 and Nwabuko et al.11 also reported a high prevalence of adults among sickle cell disease patients. However, the present study's findings contrast with those of Yahaya et al.1 and Oluwadamilola et al.18, who reported a higher prevalence of sickle cell anemia among children aged 10-20 years. The higher prevalence among individuals aged 40 years and older suggests an improvement in healthcare delivery to sickle cell patients in the study area. According to Thein et al.22, surviving beyond the age of 40 with sickle cell disease was once a remarkable exception, but today, in countries with advanced healthcare systems, the majority (over 90%) of individuals born with sickle cell disease can expect to reach adulthood. Public health measures such as universal newborn screening, penicillin prophylaxis, vaccinations and hydroxyurea therapy have led to a significant decline in sickle cell disease-related childhood mortality and morbidity in high-income countries23. Nevertheless, their lifespan remains substantially shorter than that of the general population, with a difference of over two decades22. This study found that the Yoruba ethnic group had the highest burden of sickle cell disease, followed by the Igbo group, while the Ijaw group had the lowest. This may be attributed to the larger population sizes of the Yoruba and Igbo groups in the study area. However, the scarcity of published data on sickle cell disease prevalence among Nigerian ethnic groups limits the ability to draw more detailed conclusions from this study's findings.
The findings of this study revealed that blood group O+ was the most common among the patients, accounting for 24.71%, followed by blood group A+ (23.53%), while the least was blood group AB– (1.77%). This result is consistent with the findings of most previous studies, such as those by Nwabuko et al.11 and Yahaya17 and Sacomboio et al.24, which all reported a predominance of blood group O+ among sickle cell patients. Blood group O is generally and universally common due to its status as the ancestral ABO blood group, with A and B alleles emerging in the last 20,000 years and not spreading as widely as O in the population25. Interestingly, the study also revealed that blood group O+ recorded the lowest number of severe cases, which is consistent with most previous studies, including those by Yahaya et al.1 and Amodu et al.26, which reported fewer severe cases among blood group O+. This suggests that the preponderance of blood group O+ among the patients could had been favoured by natural selection owing to its protective nature.
Regarding the genotypes of the sickle cell patients, two variants, hemoglobin SS and SC, were identified, with SS being the predominant genotype. Consistent with our findings, Yahaya et al.1 reported a higher prevalence of SS over SC in Birnin Kebbi and Nnodu et al.27, using data from the 2018 Nigeria Demographic and Health Survey, also found SS to be more dominant than SC in Nigeria. However, our study revealed a higher proportion of SC than other studies, with 9.8% of SC reported, compared to the 1.6% reported by Nnodu et al.27 and the national prevalence range of 1-3% in Nigeria11. This proportion is also higher than the 7.1% reported by Yahaya et al.1 in Birnin Kebbi, northwestern Nigeria. Studies by Nwabuko et al.11 suggest that hemoglobin SS is uniformly distributed across all geopolitical zones in Nigeria, whereas hemoglobin SC is less common and more concentrated in western Nigeria, with an estimated prevalence of 3-4%. The higher prevalence of hemoglobin SC observed in this study might indicate the presence of a modifying factor that enhances the inheritance or fitness of the SC variant or possibly a higher mutation rate from SS to SC. Further research is necessary to confirm these hypotheses.
CONCLUSION
Sickle cell anemia showed higher prevalence among females, adults aged 40+ and individuals of Yoruba and Igbo ethnicities. Blood group O+ had the highest prevalence (24.71%), with AB– the lowest (1.77%), while disease severity was greatest in AB+ and AB– patients. The HbSS was the most common variant (92.9%), with non O– blood groups showing more severe manifestations. Targeted interventions and expanded research are recommended to address these disparities and reduce severe cases.
SIGNIFICANCE STATEMENT
This study highlights critical demographic, genetic and serological disparities in sickle cell anemia (SCA) prevalence and severity. The findings reveal that SCA disproportionately affects females, adults aged 40+ and individuals of Yoruba and Igbo ethnicities. The dominance of HbSS (92.9%) and the association of non O– blood groups with severe manifestations underscore the need for targeted healthcare strategies. Moreover, blood group O+ showed the highest prevalence (24.71%), while AB+ and AB– groups exhibited greater disease severity, pointing to the potential role of blood group genetics in disease progression. These insights emphasize the importance of focused interventions and further research to mitigate the burden of SCA, particularly among vulnerable populations.
REFERENCES
- Yahaya, T.O., A.K. Attahiru, A.B. Ibrahim, M.K. Adewale, A.Z. Fari and A. Saadatu, 2024. Demographic characteristics and ABO blood group genotypes distribution among sickle cell anemia patients in Birnin Kebbi, Northwestern Nigeria. Biomorhphology J., 34: 83-92.
- Inusa, B.P.D., L.L. Hsu, N. Kohli, A. Patel, K. Ominu-Evbota, K.A. Anie and W. Atoyebi, 2019. Sickle cell disease-genetics, pathophysiology, clinical presentation and treatment. Int. J. Neonatal Screen., 5.
- Bell, V., T. Varzakas, T. Psaltopoulou and T. Fernandes, 2024. Sickle cell disease update: New treatments and challenging nutritional interventions. Nutrients, 16.
- Kato, G.J., F.B. Piel, C.D. Reid, M.H. Gaston and K. Ohene-Frempong et al., 2018. Sickle cell disease. Nat. Rev. Dis. Primers, 4.
- Ershler, W.B., L.M. de Castro, Z. Pakbaz, A. Moynahan and D. Weycker et al., 2023. Hemoglobin and end-organ damage in individuals with sickle cell disease. Curr. Ther. Res., 98.
- Kargutkar, N., M. Sawant-Mulay, P. Hariharan, S. Chandrakala and A. Nadkarni, 2023. Role of microRNA in hydroxyurea mediated HbF induction in sickle cell anaemia patients. Sci. Rep., 13.
- Onimoe, G. and S. Rotz, 2020. Sickle cell disease: A primary care update. Cleveland Clin. J. Med., 87: 19-27.
- Matthie, N., D. Ross, C. Sinha, K. Khemani, N. Bakshi and L. Krishnamurti, 2019. A qualitative study of chronic pain and self-management in adults with sickle cell disease. J. Nat. Med. Assoc., 111: 158-168.
- Osunkwo, I., H.F. O'Connor and E. Saah, 2020. Optimizing the management of chronic pain in sickle cell disease. Hematol. Am. Soc. Hematol. Educ. Program, 2020: 562-569.
- GBD 2021 SCDC, 2023. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000-2021: A systematic analysis from the Global Burden of Disease Study 2021. Lancet Haematol., 10: E585-E599.
- Nwabuko, O.C., U. Onwuchekwa and O. Iheji, 2022. An overview of sickle cell disease from the socio-demographic triangle-A Nigerian single-institution retrospective study. Pan Afr. Med. J., 41.
- Delgadinho, M., C. Ginete, B. Santos, J. Mendes, A. Miranda, J. Vasconcelos and M. Brito, 2022. Microbial gut evaluation in an angolan paediatric population with sickle cell disease. J. Cell. Mol. Med., 26: 5360-5368.
- Isa, H., E. Okocha, S.A. Adegoke, U. Nnebe-Agumadu and A. Kuliya-Gwarzo et al., 2023. Strategies to improve healthcare services for patients with sickle cell disease in Nigeria: The perspectives of stakeholders. Front. Genet., 14.
- Baldwin, Z., B. Jiao, A. Basu, J. Roth and M.A. Bender et al., 2022. Medical and non-medical costs of sickle cell disease and treatments from a us perspective: A systematic review and landscape analysis. PharmacoEconomics-Open, 6: 469-481.
- Kilonzi, M., D.L. Mwakawanga, F.F. Felician, H.J. Mlyuka and L. Chirande et al., 2022. The effects of sickle cell disease on the quality of life: A focus on the untold experiences of parents in Tanzania. Int. J. Environ. Res. Public Health, 19.
- Aleluia, M.M., T.C.C. Fonseca, R.Q. Souza, F.I. Neves and C.C. da Guarda et al., 2017. Comparative study of sickle cell anemia and hemoglobin SC disease: Clinical characterization, laboratory biomarkers and genetic profiles. BMC Hematol., 17.
- Yamane, T., 1973. Statistics: An Introductory Analysis. 3rd Edn., Harper & Row, Manhattan, New York, ISBN: 9780060473136, Pages: 1130.
- Oluwadamilola, A.D., T.I. Akinreni, M.A. Adefisan and S.D. Olayiwola, 2021. Knowledge, attitude and control practices of sickle cell diseases among senior secondary students in Osun State, Nigeria. Pan Afr. Med. J., 38.
- Adigwe, O.P., 2022. Knowledge and awareness of sickle cell disease: A cross sectional study amongst unmarried adults in Nigeria’s capital city. J. Community Genet., 13: 579-585.
- Ugwu, A.O., 2022. Gender differences in the complications of sickle cell anemia. Int. J. Med. Health Dev., 27: 38-42.
- Seck, M., M.A. Dabo, E.S. Bousso, M. Keita and S.A. Touré et al., 2024. Homozygous sickle cell disease after age of 40: Follow-up of a cohort of 209 patients in Senegal, West Africa. Adv. Hematol., 2024.
- Thein, M.S., N.E. Igbineweka and S.L. Thein, 2017. Sickle cell disease in the older adult. Pathology, 49: 1-9.
- Chaturvedi, S. and M.R. DeBaun, 2016. Evolution of sickle cell disease from a life-threatening disease of children to a chronic disease of adults: The last 40 years. Am. J. Hematol., 91: 5-14.
- Sacomboio, E.N.M., D.T. Sebastião and F. de Jesus Correia Filho Sacomboio, 2020. Sickle cell trait and blood groups (ABO and Rh) in angolans submitted to hemoglobin electrophoresis. Hematol. Oncol.: Curr. Res., 2.
- Yahaya, T.O., E.O. Oladele, M.B. Mshelia, M.O. Sifau, O.D. Fashola, M.D.A. Bunza and J. Nathaniel, 2021. Influence of ABO blood groups and demographic characteristics on the prevalence of type 2 diabetes in Lagos, Southwest Nigeria. Bull. Nat. Res. Cent., 45.
- Amodu, O.K., S.A. Olaniyan, A.A. Adeyemo, M. Troye-Blomberg, P.E. Olumese and O.O. Omotade, 2012. Association of the sickle cell trait and the ABO blood group with clinical severity of malaria in Southwest Nigeria. Acta Trop., 123: 72-77.
- Nnodu, O.E., A.P. Oron, A. Sopekan, G.O. Akaba, F.B. Piel and D.L. Chao, 2021. Child mortality from sickle cell disease in Nigeria: A model-estimated, population-level analysis of data from the 2018 demographic and health survey. Lancet Haematol., 8: E723-E731
How to Cite this paper?
APA-7 Style
Tajudeen,
Y., Kehinde,
A.M., Oke,
O., Akinpelu,
M., Koko,
D.J., Muhammad,
U.B. (2025). Demographic Characteristics and ABO Blood Group Genotype Distribution among Sickle Cell Anaemia Patients in Lagos, Southwest Nigeria. Asian Journal of Biological Sciences, 18(1), 152-158. https://doi.org/10.3923/ajbs.2025.152.158
ACS Style
Tajudeen,
Y.; Kehinde,
A.M.; Oke,
O.; Akinpelu,
M.; Koko,
D.J.; Muhammad,
U.B. Demographic Characteristics and ABO Blood Group Genotype Distribution among Sickle Cell Anaemia Patients in Lagos, Southwest Nigeria. Asian J. Biol. Sci 2025, 18, 152-158. https://doi.org/10.3923/ajbs.2025.152.158
AMA Style
Tajudeen
Y, Kehinde
AM, Oke
O, Akinpelu
M, Koko
DJ, Muhammad
UB. Demographic Characteristics and ABO Blood Group Genotype Distribution among Sickle Cell Anaemia Patients in Lagos, Southwest Nigeria. Asian Journal of Biological Sciences. 2025; 18(1): 152-158. https://doi.org/10.3923/ajbs.2025.152.158
Chicago/Turabian Style
Tajudeen, Yahaya, Adewale Mutiyat Kehinde, Olamide Oke, Moronkeji Akinpelu, Danjuma Jamilu Koko, and Usman Bello Muhammad.
2025. "Demographic Characteristics and ABO Blood Group Genotype Distribution among Sickle Cell Anaemia Patients in Lagos, Southwest Nigeria" Asian Journal of Biological Sciences 18, no. 1: 152-158. https://doi.org/10.3923/ajbs.2025.152.158

This work is licensed under a Creative Commons Attribution 4.0 International License.