Multidrug Resistance of Bacteria Causing Enteric Infections in Patients with Arterial Hypertension at the Douala Laquintinie Hospital in Cameroon
-
Ornella Djiolieu Tsobeng
Department of Biochemistry, Faculty of Science, University of Dschang, Dschang, Cameroon
Michael Francis KengneDepartment of Biochemistry, Faculty of Science, University of Dschang, Dschang, Cameroon
Ballue Serges Tatiefo DadjoDepartment of Biochemistry, Faculty of Science, University of Dschang, Dschang, Cameroon
Victor Kuete

Department of Biochemistry, Faculty of Science, University of Dschang, Dschang, Cameroon
| Received 23 Sep, 2024 |
Accepted 19 Dec, 2024 |
Published 30 Jun, 2025 |
Background and Objective: Hypertension is a worldwide public health problem. Numerous studies have shown the links between hypertension and bacterial infections. The imbalance of intestinal microbiota observed in hypertensive patients exposes them to bacterial infections resistant to several antibiotics. This study aims to determine the resistance profile of pathogenic enterobacteria in hypertensive and non-hypertensive patients at the Laquintinie Hospital in Douala (Cameroon). Materials and Methods: Stool samples from 327 hypertensive patients and 191 non-hypertensive patients, suffering from enteric disorders were collected to isolate pathogenic intestinal bacteria using selective and differential culture media. Their susceptibility profile was determined by the antibiogram. The statistical analyses were performed using Epi InfoTM software version 7.2.4. The Chi-square test was used to compare the frequencies of multidrug-resistant enterobacteria in hypertensive and non-hypertensive patients. The relationship between resistance profile and hypertension was performed using the visual dashboard test. Results: The frequency of hypertension was higher in women (60.24%) than in men (39.76%). All bacteria were isolated predominantly from hypertensive patients who have undergone antihypertensive treatment. The antimicrobial susceptibility test revealed thatthe resistance of K. pneumoniae, P. mirabilis and Proteus vulgarisisolates to AMC, SXT a nd multidrug resistance of K. pneumoniae (p = 0.033) and K. oxytoca (p = 0.001) was significantly higher in hypertensive than non-hypertensive patients. Conclusion: These results underline the need for the prevention and management of enteric infections in hypertensive patients.
| Copyright © 2025 Tsobeng et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Hypertension (high blood pressure) is a chronic medical condition in which blood pressure is elevated1. It is the most common cardiovascular disorder, affecting around one billion people worldwide and remains the major contributor to the global burden of disease and mortality2. Several studies have linked hypertension to the gut microbiota. These studies have shown that altered gut microbiota is a causal factor in the development of hypertension and that hypertension causes an imbalance in gut flora3-5. Yang et al.4 have shown that hypertension may lead to dysfunction of the intestinal barrier, with an increase in harmful bacteria and a decrease in beneficial bacteria. It is important to remember that the main function of the intestinal microbiota is to protect the gut against colonization by exogenous pathogens and potentially harmful microorganisms6. The dysbiosis observed in hypertensive patients therefore exposes them to enteric infections with resistant bacteria7. In addition, antihypertensives, mainly of the angiotensin-converting enzyme (ACE) inhibitor class, are also thought to play a role in weakening the immune system, reducing its ability to defend against bacterial infections. However, it has been shown that hypertensive patients with asymptomatic bacteriuria are exposed to high rates of multidrug resistance to Klebsiella spp.8 (100%), Proteus spp. (100%) and E. coli (92.30%). Bacterial infections caused by enterobacteria, which are resistant to all current classes of antimicrobial drugs, have become a serious problem in the fight against bacterial infections in public health9. All parts of the world have seen dangerously high levels of antibiotic resistance and new resistance mechanisms are appearing and spreading everywhere, endangering the ability to treat common infectious diseases10. Although numerous studies have been carried out on arterial hypertension, the association between resistance in pathogenic enterobacteria and arterial hypertension is still unknown. In Cameroon, there is a dearth of data on this public health problem. Consequently, this study aims to determine the relationship between the resistance profile of pathogenic enterobacteria, arterial hypertension and its treatment.
MATERIALS AND METHODS
Study design: This is a cross-sectional study carried out from June, 2022 to June, 2023 at the Laquintinie Hospital in Douala, located in the Littoral Region of Cameroon. It is one of the reference centers that houses a Cardiology Department in Douala, Cameroon.
Population studied: This study focused on hypertensive and non-hypertensive patients with enteric disorders. The 518 people signed informed consent to participate in this study. The 327 patients were hypertensive and 191 were non-hypertensive. Patients whose physicians had prescribed coproculture and who had not received any antibiotics were included. In addition, fifteen patients who were seropositive for Human Immunodeficiency Virus (HIV) and seropositive for hepatitis B and C were excluded. Pregnant women and patients who had not signed an informed consent form to participate in this study were not included.
Ethical approval: Ethical clearance was obtained from The Institutional Ethics Committee for Research on Human Health of the University of Douala (Littoral, Cameroon) (CEI-UDo), N°3130CEI-Udo/06/2022/T. Subsequently, administrative authorization was obtained from the Director of Laquintinie Hospital and Consent (from adults) or consent and assent (for participants<21 years) were obtained. The study design was explained to the patients and a signed informed consent to participate in the study was obtained from each patient. A questionnaire was administered to each patient, collecting information on age, gender and socio-demographic data for this study.
Blood pressure measurement: Systolic and diastolic blood pressure readings were taken on patients who had previously been declared hypertensive by the cardiologist, as well as on non-hypertensive patients. Three blood pressure readings were taken on each patient and the average of these three readings was used in this study. Measurements were taken on the patient in a seated position, after 5 min rest, using a full-screen electronic blood pressure monitor (OMROM 705).
Stool sample collection: The 518 stool samples were taken by the patients in the laboratory of Laquintinie Hospital. The patient was not on antibiotics beforehand and complied with the following instructions: Wash hands. Urinate before collection, stools must not be spoiled by urine. Collect part of the stool (especially the muco-purulent or bloody parts) using the spatula in the bottle supplied by the laboratory. The stools collected in the sterile vials (Deltalab 409552 PK, Belgium) were then transported to the laboratory’s Bacteriology Department using a cooler suitable for this type of transport.
Isolation and identification of bacteria: Stool samples from each participant were immediately transported to the laboratory for culture. After diluting a fraction of the stool in physiological saline until an opalescent suspension was obtained, a suspension of stool sample was collected with a platinum loop (RENONLAB, Shanghai, China) and streaked onto Salmonella-Shigella (SS) agar (Titan Biotech Ltd., Rajasthan, India), Hektoen enteric agar (Becton Dickinson-Difco, Franklin Lakes, New Jersey, USA) and eosin-methylene blue agar (EMB) (Titan Biotech Ltd., Rajasthan, India). The plates were incubated at 37°C for 24 hrs. After incubation, bacterial isolates were purified on nutrient agar (Titan Biotech Ltd., Rajasthan, India). Gram staining was carried out to confirm that the bacteria isolated were gram-negative. These bacteria appeared under the microscope (Olympus Cx22, Shanghai, China) as pink-stained rods. Bacterial isolates were identified based on their morphological characteristics and using the API 20 E Gallery (Biomérieux, Lyon, France).
Antibiotic susceptibility test: In vitro susceptibility testing of bacterial isolates to various commonly used antibiotics was carried out using the Kirby-Bauer diffusion method11. Antibiotics tested included the penicillins (amoxicillin (AMO, 10 μg); amoxicillin/clavuranic acid (AMC, 20/10 μg)); cephalosporins (ceftriaxone (CRO, 30 μg); cefepime (CPM, 50 μg); cefotaxime (CTX, 5 μg)); monobactams (aztreonam (ATM, 50 μg)); carbapenems (imipenem (IMP, 10 μg)); fluoroquinolones (Ciprofloxacin (CIP, 5 μg); ofloxacin (OFX, 10 μg); nalixidic acid (NAL, 10 μg)); aminoglycosides (amikacin (AMK, 30 μg); gentamycin (GEN, 50 μg)); fosfomycin (FOS, 200 μg) and trimethoprim-sulfamethoxazole (SXT, 25 μg) (Singapore Biosciences PTE Ltd., Singapore). Briefly, the bacterial isolate tested was emulsified in physiological saline until turbidity was similar to that of the 0.5% McFarland standard. Approximately 15-20 mL of the prepared Mueller-Hinton agar (MHA) (Titan Biotech Ltd., Rajasthan, India) was aseptically poured into a 90 mm Petri dish (JLY-PYM-001, Goldenwell Ltd., Shanghai, China). After solidification, MHA underwent sterility and fertility tests to ensure that the culture medium had been properly prepared and had not been contaminated during preparation. After confirmation, the agar was inoculated with a sterile swab to obtain a semi-fluent growth, followed by the deposition of the antibiotic discs. The assembly was then incubated at 37°C for 24 hrs. Following incubation, the Clinical and Laboratory Standards Institute (CLSI) criteria were used to measure and interpret the zones of inhibition surrounding the antibiotic discs11. Escherichia coli ATCC 25922 was used to ensure the quality control of the antibiotic discs (Singapore Biosciences PTE Ltd., Singapore), media and incubation conditions. Multidrug-resistant (MDR) bacteria were those that exhibited resistance to three or more antibiotic families9,12.
Statistical analysis: The Chi-square test was used to compare the frequencies of pathogenic enterobacteria and multidrug-resistant enterobacteria in hypertensive and non-hypertensive patients. A value of p<0.05 was considered significant. The visual dashboard test was used to compare odds ratios at a 95% confidence interval (CI) of enterobacterial resistance in the different groups, to infer a possible relationship between resistance profile and arterial hypertension. All these analyses were performed using Epi InfoTM software version 7.2.4 (CDC, Atlanta, USA).
RESULTS
Of a total of 518 hypertensive and non-hypertensive patients with enteric disorders, 211 (40.3%) were men and 307 (59.27%) were women. Among the men, 130 (39.76%) were hypertensive and 81 (42.41%) were non-hypertensive. Among the women, 197 (60.24%) were hypertensive and 110 (57.59%) were non-hypertensive. Patients suffering from hypertension were older than non-hypertensive patients. A significant number of hypertensive patients were observed in the age groups 60 to<80 years (84.41%; p<0.001) and ≥ 80 years (77.77%; p = 0.189). Whereas a significant number of non-hypertensive patients were observed in the age group 20 to<40 years (81.48%; p<0.001). The mean age of study patients was significantly higher (p<0.001) in hypertensive patients than in non-hypertensive patients (43.45±15.54). With systolic and diastolic blood pressure significantly higher (p<0.001) in hypertensive than in non-hypertensive patients (Table 1).
|
|
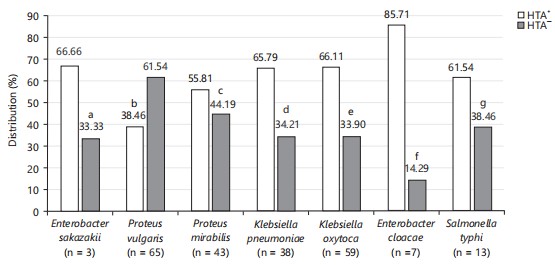
In the present study, infection rates of Enterobacter cloacae (85.71 vs 14.29%, p = 0.212), Klebsiella oxytoca (66.10 vs 33.89%, p = 0.614), Klebsiella pneumoniae (65.79 vs 34.21%, p = 0.723), Salmonella typhi (61.54 vs 38.46%, p = 0.384) and Proteus mirabilis (55.81 vs 44.19%, p = 0.299) were higher in hypertensive than non-hypertensive patients. In contrast, infection rate of Proteus vulgaris (61.54 vs 38.46% p<0.001) was the most frequent in non-hypertensive patients (Fig. 1).
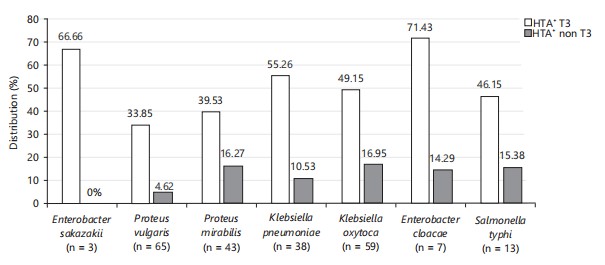
Among the hypertensive population (n = 237), 244 were on antihypertensive treatment and 83 were without antihypertensive treatment. (Fig. 2) showed the distribution of pathogenic enterobacteria according to treatments for hypertension. A greater proportion of all bacteria were isolated from hypertensive patients who have undergone antihypertensive treatments than those without antihypertensive treatment.
| Table 1: | Demographic characteristics of hypertensive and non-hypertensive patients with enteric disorders | |||
| Parameters | HTA+ with enteric disorders n=327 (%) |
HTA– with enteric disorders n=191 (%) |
p-value | |
| Sex | Male (n=211) | 130 (39.76) | 81 (42.41) | 0.553 |
| Female (n = 307) | 197 (60.24) | 110 (57.59) | ||
| Age groups (years) | 20-40 ( n = 108) | 20 (18.52) | 88 (81.48) | <0.001 |
| 40-60 ( n = 206) | 136 (66.02) | 70 (36.65) | 0.267 | |
| 60-80 (n = 186) | 157 (84.41) | 29 (15.59) | <0.001 | |
| >80; n = 18 | 14 (77.77) | 4 (33.33) | 0.189 | |
| Mean age; Mean±SD | Total | 59.54±12.14 (32-88) | 43.45±15.54 (20-87) | <0.001 |
| (min-max) | Male | 58.13±12.18 (32-87) | 43.30±13.43 (20-87) | <0.001 |
| Female | 60.46±12.05 (33-88) | 43.56±16.98 (20-84) | <0.001 | |
| Blood pressure | SBP; Mean±SD (min-max) | 165.44±25.74 (102-269) | 119.30±11.36 (80-152) | <0.001 |
| DBP; Mean±SD (min-max) | 99.63±17.94 (58-117) | 77.57±11.12 (49-110) | <0.00 | |
| Pulsation; Mean±SD (min-max) | 87.20±16.40 (42-154) | 82.71±13.83 (46-110) | 0.001 | |
| SBP: Systolic blood pressure, DBP: Diastolic blood pressure, HTA+: Hypertensive patients, HTA–: Non-hypertensive patients, n: Number of patients, min: Minimum and max: Maximum | ||||
Depending on hypertension status, Klebsiella pneumoniae, Proteus mirabilis and Proteus vulgaris isolates showed higher resistance rates to AMC (68; 66.67; 48.00% vs 30.77; 57.80; 40.00%), FOS (48.00; 50.00; 48.00% vs 38.46; 47.37; 25.00%) and SXT (64.00; 50.00; 52.00% vs 38.46; 15.79; 22.50%) in hypertensive than non-hypertensive patients. Klebsiella oxytoca, Klebsiella pneumoniae, Proteusmirabilis and Proteus vulgaris isolates showed resistance rates to NAL ranging from 45 to 65% in non-hypertensive patients and from 28 to 51.28% in hypertensive patients. Salmonella typhi isolates showed higher resistance rates to AMC (87.50 vs 20.00%), CRO (75.00 vs 60.00%) and CPM (62.50 vs 20.00%) in hypertensive than non-hypertensive patients. Enterobacter cloacae isolates showed higher resistance rates to NAL (100 vs 50%), CRO (100 vs 66.67%) and CPM (100 vs 66.67%), respectively, in non-hypertensive than in hypertensive patients. Salmonella typhi, Enterobacter sakazakii and Enterobacter cloacae isolates showed high resistance rates to AMO in patients suffering from hypertension (75; 100; 83.33%) and in non-hypertensive patients (80; 100; 100%). K. oxytoca, K. pneumoniae, P mirabilis, P. vulgaris and S. typhi isolates showed high levels of sensitivity to IMP, AMK and GEN in both hypertensive (84.62; 96.00; 70.83; 80.00; 75.00%) and non-hypertensive patients (100, 100; 73.68; 92.50; 100%) (Table 2).
Depending on hypertension status, multidrug resistance of Kelbsiella pneumoniae (p = 0.033) and Klebsiella oxytoca (p = 0.001) was significantly higher in hypertensive than non-hypertensive patients. Proteus mirabilis, Enterobacter cloacae and Salmonella typhi isolates also showed higher multidrug resistance rates in hypertensive (75; 83.33; 87.50; 100%) than in non-hypertensive patients (57.89; 0; 80; 95.65%) (Table 3).
The association between the resistance of pathogenic bacterial isolates and hypertension is shown in Table 4. Resistance of Klebsiella oxytoca (OR: 6.72; 95% CI: 1.94-23.18); Klebsiella pneumoniae (OR: 4.66: 95% CI: 1.07-20.21) and Proteus mirabilis (OR: 2.18; 95% CI: 0.59-7.98) to several antibiotics was strongly correlated with arterial hypertension.
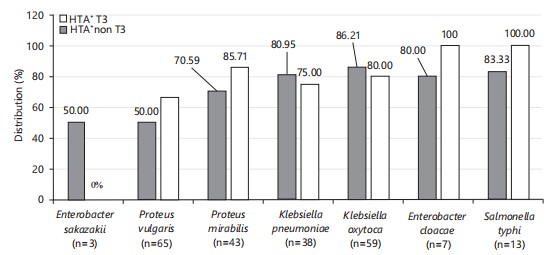
Klebsiella oxytoca, Klebsiella pneumoniae and Enterobacter sakazakii isolates showed higher multidrug resistance rates in hypertensive patients who have undergone antihypertensive treatment (86.21%; 80.95; 50.00%) than those without antihypertensive treatment (80.00; 75.00; 0.00%). In untreated hypertensive patients, isolates of Proteus mirabilis, Enterobacter cloacae and Salmonella typhi showed highest rates of multidrug resistance (85.71; 100; 100%) (Fig. 3).
Table 5 hows the association between co-infection and hypertension. It appears that Proteus-Klebsiella spp., co-infection was the most frequent in the study population, with a higher frequency in hypertensive patients (53.33%) than in non-hypertensive patients (46.67%). Enterobacter-Klebsiella spp., co-infection and Enterobacter-Proteus spp., co-infections were only observed in hypertensive patients (100%; p>0.05). On the other hand, Salmonella-Klebsiella spp., co-infection was morecommon in non-hypertensive patients (66.67%) than hypertensive patients (33.33%). Overall, co-infection was more prevalent in hypertensive patients (60.00%) than in non-hypertensive patients (40.00%).
| Table 2: | Susceptibility profile of isolated bacteria in hypertensive and non-hypertensive patients | |||
| Bacteria, patients, number of isoates, susceptibility profiles and percentage in bracket | |||||||||||||||
| Klebsiella oxytoca | Klebsiella pneumoniae | Proteus mirabilis | Proteus vulgaris | Salmonella typhi | Cronobacter sakazakii | Enterobacter cloacae | |||||||||
| Antibiotics | Susceptibility profile |
HTA+ (n=39) (%) |
HTA– (n=20) (%) |
HTA+ (n=25) (%) |
HTA– (n=13) (%) |
HTA+ (n=24) (%) |
HTA– (n=19) (%) |
HTA+ (n=25) (%) |
HTA– (n=40) (%) |
HTA+ (n=8) (%) |
HTA– (n=5) (%) |
HTA+ (n=2) (%) |
HTA– (n=1) (%) |
HTA+ (n=6)(%) |
HTA– (n=1) (%) |
| IMP | R | 3 (7.69) | 0 (0.00) | 1 (4.00) | 0 (0.00) | 3 (12.50) | 1 (5.26) | 2 (8.00) | 3 (7.50) | 2 (25.00) | 0 (0.00) | 1 (50.00) | 0 (0.00) | 3 (50.00) | 0 (0.00) |
| I | 3 (7.69) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 4 (16.67) | 4 (21.05) | 3 (12.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 33 (84.62) | 20 (100) | 24 (96.00) | 13 (100) | 17 (70.83) | 14 (73.68) | 20 (80.00) | 37 (92.50) | 6 (75.00) | 5 (100) | 1 (50.00) | 1 (100) | 3 (50.00) | 1 (100) | |
| AMO | R | 37 (94.87) | 18 (90.00) | 22 (88.00) | 11 (84.62) | 19 (79.17) | 16 (84.21) | 22 (88.00) | 27 (67.50) | 6 (75.00) | 4 (80.00) | 2 (100) | 1 (100) | 5 (83.33) | 1 (100) |
| I | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (5.26) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 2 (5.13) | 2 (10.00) | 3 (12.00) | 2 (15.38) | 5 (20.83) | 2 (10.53) | 3 (12.00) | 13 (32.50) | 2 (25.00) | 1 (20.00) | 0 (0.00) | 0 (0.00) | 1(16.67) | 0 (0.00) | |
| CTX | R | 22 (56.41) | 6 (30.00) | 8 (32.00) | 6 (46.15) | 10 (41.67) | 9 (47.37) | 11 (44.00) | 16 (40.00) | 3 (37.50) | 3 (60.00) | 0 (0.00) | 0 (0.00) | 2 (33.33) | 0 (0.00) |
| I | 0 (0.00) | 1 (5.00) | 0 (0.00) | 1 (7.69) | 2 (8.33) | 0 (0.00) | 1 (4.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (50.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 17 (43.59) | 13 (65.00) | 17 (68.00) | 6 (46.15) | 12 (50.00) | 10 (52.63) | 13 (52.00) | 24 (60.00) | 5 (62.50) | 2 (40.00) | 1 (50.00) | 1 (100) | 4 (66.67) | 1 (100) | |
| CPM | R | 20 (51.28) | 6 (30.00) | 7 (28.00) | 4 (30.77) | 15 (62.50) | 11 (57.89) | 6 (24.00) | 16 (40.00) | 5 (62.50) | 1 (20.00) | 1 (50.00) | 0 (0.00) | 2 (33.33) | 1 (100) |
| I | 3 (7.69) | 0 (0.00) | 2 (8.00) | 0 (0.00) | 1 (4.17) | 1 (5.26) | 1 (4.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 16 (41.03) | 14 (70.00) | 16 (64.00) | 9 (69.23) | 8 (33.33) | 7 (36.84) | 18 (72.00) | 24 (60.00) | 3 (37.50) | 4 (80.00) | 1 (50.00) | 1 (100) | 4 (66.67) | 0 (0.00) | |
| CRO | R | 27 (69.23) | 9 (45.00) | 13 (52.00) | 7 (53.85) | 9 (37.50) | 12 (63.16) | 10 (40.00) | 15 (37.50) | 6 (75.00) | 3 (60.00) | 0 (0.00) | 1 (100) | 4 (66.67) | 1 (100) |
| I | 1 (2.56) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 3 (7.50) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 11 (28.21) | 11 (55.00) | 12 (48.00) | 6 (46.15) | 15 (62.50) | 7 (36.84) | 15 (60.00) | 22 (55.00) | 2 (25.00) | 2 (40.00) | 2 (100) | 0 (0.00) | 2 (33.33) | 0 (0.00) | |
| AMC | R | 31 (79.49) | 5 (25.00) | 17 (68.00) | 4 (30.77) | 16 (66.67) | 11 (57.89) | 12 (48.00) | 16 (40.00) | 7 (87.50) | 3 (60.00) | 1(50.00) | 1 (100) | 2 (33.33) | 0 (0.00) |
| I | 1 (2.56) | 1 (5.00) | 0 (0.00) | 1 (7.69) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 1 (2.50) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 7 (17.95) | 14 (70.00) | 8 (32.00) | 8 (61.54) | 8 (33.33) | 8 (42.11) | 13 (52.00) | 23 (57.50) | 1 (12.50) | 2 (40.00) | 1 (50.00) | 0 (0.00) | 4 (66.67) | 1 (100) | |
| FOS | R | 20 (51.28) | 3 (15.00) | 12 (48.00) | 5 (38.46) | 12 (50.00) | 9 (47.37) | 12 (48.00) | 10 (25.00) | 3 (37.50) | 2 (40.00) | 1(50.00) | 0 (0.00) | 5 (83.33) | 0 (0.00) |
| I | 0 (0.00) | 1 (5.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| ATM | R | 18 (46.15) | 5 (25.00) | 8 (32.00) | 5 (38.46) | 10 (41.67) | 5 (26.32) | 7 (28.00) | 11 (27.50) | 4 (50.00) | 3 (60.00) | 0 (0.00) | 1 (100) | 1 (16.67) | 0 (0.00) |
| I | 1 (2.56) | 0 (0.00) | 2 (8.00) | 1 (7.69) | 3 (12.50) | 1 (5.26) | 3 (12.00) | 4 (10.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 20 (51.28) | 15 (75.00) | 15 (60.00) | 7 (53.85) | 11 (45.83) | 13 (68.42) | 15 (60.00) | 25 (62.50) | 4 (50.00) | 2 (40.00) | 2 (100) | 0 (0.00) | 5 (83.33) | 1 (100) | |
| SXT | R | 32 (82.05) | 7 (35.00) | 16 (64.00) | 5 (38.46) | 12 (50.00) | 3 (15.79) | 13 (52.00) | 9 (22.50) | 5 (62.50) | 3 (60.00) | 1 (50.00) | 1 (100) | 4 (66.67) | 0 (0.00) |
| I | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 2 (8.00) | 3 (7.50) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 7 (17.95) | 13 (65.00) | 9 (36.00) | 8 (61.54) | 12 (50.00) | 15 (78.95) | 10 (40.00) | 28 (70.00) | 3 (37.50) | 2 (40.00) | 1 (50.00) | 0 (0.00) | 2 (33.33) | 1 (100) | |
| NAL | R | 20 (51.28) | 13 (65.00) | 13 (52.00) | 7 (53.85) | 10 (41.67) | 10 (52.63) | 7 (28.00) | 18 (45.00) | 2 (25.00) | 5 (100) | 0 (0.00) | 0 (0.00) | 3 (50.00) | 1 (100) |
| I | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 19 (48.72) | 7 (35.00) | 12 (48.00) | 6 (46.15) | 14 (58.33) | 9 (47.37) | 18 (72.00) | 22 (55.00) | 6 (75.00) | 0 (0.00) | 2 (100) | 1 (100) | 3 (50.00) | 0 (0.00) | |
| AMK | R | 11 (28.21) | 3 (15.00) | 8 (32.00) | 3 (23.08) | 6 (25.00) | 7 (36.84) | 4 (16.00) | 9 (22.50) | 2 (25.00) | 1 (20.00) | 1 (50.00) | 0 (0.00) | 3 (50.00) | 0 (0.00) |
| I | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 28 (71.79) | 17 (85.00) | 17(68.00) | 10 (76.92) | 18 (75.00) | 12 (63.16) | 21 (84.00) | 31 (77.50) | 6 (75.00) | 4 (80.00) | 1 (50.00) | 1 (100) | 3 (50.00) | 1 (100) | |
| GEN | R | 8 (20.51) | 1 (5.00) | 6 (24.00) | 2 (15.38) | 0 (0.00) | 1 (5.26) | 0 (0.00) | 4 (10.00) | 2 (25.00) | 0 (0.00) | 1 (50.00) | 0 (0.00) | 1 (16.67) | 0 (0.00) |
| I | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 31 (79.49) | 19 (95.00) | 19 (76.00) | 11 (84.62) | 24 (100) | 18 (94.74) | 25 (100) | 36 (90.00) | 6 (75.00) | 5 (100) | 1 (50.00) | 1 (100) | 5 (83.33 | 1 (100) | |
| OFX | R | 22 (56.41) | 4 (20.00) | 16 (64.00) | 7 (53.85) | 11 (45.83) | 11 (57.89) | 7 (28.00) | 11 (27.50) | 5 (62.50) | 3 (60.00) | 0 (0.00) | 0 (0.00) | 1 (16.67) | 0 (0.00) |
| I | 0 (0.00) | 2 (10.00) | 4 (16.00) | 1 (7.69) | 2 (8.33) | 0 (0.00) | 0 (0.00) | 4 (10.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 17 (43.59) | 14 (70.00) | 5 (20.00) | 5 (38.46) | 11 (45.83) | 8 (42.11) | 18 (72.00) | 25 (62.50) | 3 (37.50) | 2 (40.00) | 2 (100) | 1 (100) | 5 (83.33) | 1 (100) | |
| CIP | R | 20 (51.28) | 4 (20.00) | 14 (56.00) | 7 (53.85) | 11 (45.83) | 8 (42.11) | 7 (28.00) | 12 (30.00) | 3 (37.50) | 3 (60.00) | 1 (50.00) | 1 (100) | 3 (50.00) | 0 (0.00) |
| I | 1 (2.56) | 2 (10.00) | 2 (8.00) | 1 (7.69) | 1 (4.17) | 1 (5.26) | 1 (4.00) | 3 (7.50) | 0 (0.00) | 1 (20.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| S | 18 (46.15) | 14 (70.00) | 9 (36.00) | 5 (38.46) | 12 (50.00) | 10 (52.63) | 17 (68.00) | 25 (62.50) | 5 (62.50) | 1 (20.00) | 1 (50.00) | 0 (0.00) | 3 (50.00) | 1 (100) | |
| AMO : Amoxicillin, CIP: Ciprofloxacin, CRO: Ceftriaxone, CTX: Cefotaxime, IMP: Imipenem, FOS : Fosfomycin, AMC: Amoxicillin+clavunalic acid, CPM: Cefepime, S: Susceptible, I: Intermediate, R: Resistant, n: Number of bacterial isolates, HTA+: Hypertensive patients, HTA: Non-hypertensive patients, OFX: Ofloxacin, CIP: Ciprofloxacin, GEN: Gentamicin, NAL: Nalidixic acid, SXT: Trimethoprim-sulphamethoxazole, AMK: Amikacin, ATM: Aztreonam, S: Susceptible, I: Intermediate, R: Resistant, n: Frequency, HTA+: Hypertensive patients and HTA: Non-hypertensive patient | |||||||||||||||
|
| Table 3: | Relationship between bacterial resistance, MDR and hypertension status | |||
| HTA+ n (%) | HTA– n (%) | |||||
| Bacteria | Resistant | MDR | Resistant | MDR | χ2 | p-value |
| Enterobacter sakazakii (n = 3) | 1 (50.00) | 1(50.00) | 0 (0.00) | 1 (100) | 0.75 | 0.384 |
| Proteus vulgaris (n = 65) | 12 (48.00) | 13 (52.00) | 24 (60.00) | 16 (40.00) | 0.89 | 0.343 |
| Proteus mirabilis (n = 43) | 6 (25.00) | 18 (75.00) | 8 (42.11) | 11 (57.89) | 1.41 | 0.234 |
| Klebsiella pneumoniae (n = 38) | 5 (20.00) | 20 (80.00) | 7 (53.85) | 6 (46.15) | 4.53 | 0.033 |
| Klebsiella oxytoca (n = 59) | 6 (15.38) | 33 (84.62) | 11 (55.00) | 9 (45.00) | 10.11 | 0.001 |
| Enterobacter cloacae (n = 7) | 1 (16.67) | 5 (83.33) | 1 (100) | 0 (0.00) | 2.91 | 0.087 |
| Salmonella typhi (n = 13) | 1 (12.50) | 7 (87.50) | 1 (20.00) | 4 (80.00) | 0.13 | 0.715 |
| HTA+: Hypertensive patients, HTA–: Non-hypertensive patients, MDR: Multidrug-resistant, χ2: Chi-square and n: Number of bacterial isolates | ||||||
| Table 4: | Odds ratio of bacterial resistance in hypertensive patients | |||
| Hypertension | ||
| Baterial isolates | OR | 95% CI |
| Enterobacter sakazakii | 0.00 | ND |
| Proteus vulgaris | 1.62 | 0.59-4.45 |
| Proteus mirabilis | 2.18 | 0.59-7.98 |
| Klebsiella pneumoniae | 4.66 | 1.07-20.21 |
| Klebsiella oxytoca | 6.72 | 1.94-23.18 |
| Enterobacter cloacae | 0.00 | ND |
| Salmonella typhi | 1.75 | 0.08-36.28 |
| ND: Not defined, OR: Odds ratio and CI: Confidence interval | ||
| Table 5: | Association between co-infection and hypertension | |||
| Bacterial co-infection | HTA+ (%) | HTA– (%) | p-value |
| Salmonella+Klebsiella spp. (n = 3) | 1 (33.33) | 2 (66.67) | 0.283 |
| Proteus+Salmonella typhi (n = 2) | 1 (50.00) | 1 (50.00) | 0.699 |
| Proteus+Klebsiella spp. (n = 15) | 8(5.33) | 7 (46.67) | 0.424 |
| Enterobacter+Klebsiella spp. (n = 3) | 3 (100) | 0 (0.00) | 0.184 |
| Enterobacter+Proteus spp. (n = 2) | 2 (100) | 0 (0.00) | 0.278 |
| Total of co-infection (n = 25) | 15 (60.00) | 10 (40.00) | 0.11 |
| HTA+: Hypertensive patients, HTA–: Non-hypertensive patients and n: Number of bacterial isolates | |||
DISCUSSION
In this study the incidence of hypertension was higher in women (60.24%) than in men (39.76%). This was contrary to the studies carried out by two other research teams13,14. This slight increase in the prevalence of hypertension in women could be explained by certain risk factors (advanced age, low level of education and high body mass index) that are associated with this increase, as demonstrated by Choi et al.15. Patients suffering from hypertension in this study were older than non-hypertensive patients. A significant number of hypertensive patients were observed in the age groups 60 to<80 years (84.41%; p<0.001) and≥80 years (77.77%; p = 0.189). This result was comparable to that of Baiting Liu et al.16, in which the prevalence of hypertension was high in patients aged 70 to 79 years (75.10%) and 80 to 99 years (73.60%). This demonstrated that age is one of the risk factors for hypertension, as age increases, so does the likelihood of developing hypertension14,17.
Bacterial infections still represent a worldwide public health problem18-20. This study showed that infection rates of Enterobacter cloacae (85.71 vs 14.29% p = 0.212), Klebsiella oxytoca (66.10 vs 33.89%, p= 0.614), Klebsiella pneumoniae (65.79 vs 34.21%, p = 0.723), Salmonella typhi (61.54 vs 38.46%, p = 0.384) and Proteus mirabilis (55.81 vs 44.19%, p = 0.299) were higher in hypertensive than non-hypertensive patients. Several studies have already demonstrated that the bacteria isolated above are pathogens responsible for infections in humans21,22. The predominance of these bacteria in hypertensive patients could be explained by dysbiosis of the gut microbiota, characterized by a reduction in bacterial biodiversity and vulnerability of immune function compared to non-hypertensive patients4-6.
Depending on the treatment of hypertension, all the bacteria (Proteus vulgaris, Klebsiella oxytoca, Proteus mirabilis, Klebsiella pneumoniae, Enterobacter cloacae, Enterobacter sakazakii and Salmonella typhi) were more frequently isolated from hypertensive patients who had undergone antihypertensive treatments than those without hypertensive treatments. This finding suggested that antihypertensive drugs may play a role in exposing hypertensive patients to certain bacterial infections. This may be justified by previously reported data that demonstrated that antihypertensives play a role in weakening the immune system, thus exposing them to bacterial infections7.
Antibiotic resistance is a major global threat to public health22. The antimicrobial susceptibility test revealed that Klebsiella pneumoniae, Proteus mirabilis and Proteus vulgaris isolates showed higher rates of resistance to AMC, FOS and SXT in hypertensive than non-hypertensive patients. These results were similar to those of Odetoyin and his collaborators8. Salmonella typhi isolates showed higher rates of resistance to AMC, CRO and CPM in hypertensive than non-hypertensive patients. The high resistance observed in this study to AMC means their frequent usage may be a contributing factor in the proliferation of Enterobacteriaceae and the development of resistant strains in the gastrointestinal tract23. Salmonella typhi, Enterobacter sakazakii and Enterobacter cloacae isolates showed high resistance rates to AMO in patients suffering from hypertension (75; 100; 83.33%) and in non-hypertensive patients (80; 100; 100%). Enterobacteriaceae have developed high resistance to Penicillins via production of penicillinase24, this explains high resistance to AMO observed in this study. K. oxytoca, K. pneumoniae, P. mirabilis, P. vulgaris and S. typhi isolates showed high levels of sensitivity to AMK and GEN in both hypertensive and non-hypertensive patients. This good sensitivity towards antibiotics from the aminoglycoside family (GEN and AMK) could be explained by the limited use and unavailability of the local market of these molecules.
In this study, multidrug resistance was defined as the resistance of an isolate to three or more families of antibiotics25. Bacterial resistance to multiple antibiotics has reached dangerously high levels worldwide10,26. Depending on hypertension status, multidrug resistance of Klebsiella pneumoniae (p = 0.033) and Klebsiella oxytoca (p = 0.001) was significantly higher in hypertensive than non-hypertensive patients. This high level of multidrug resistance may be due to inadequate and excessive antibiotic consumption without a medical prescription. Isolates of Proteus mirabilis, Enterobacter cloacae and Salmonella typhi also showed higher rates of multidrug resistance in hypertensive patients than in non-hypertensive patients. These results corroborated those of Odetoyin et al.8 who revealed high multidrug resistance rates of Klebsiella and Proteus spp., in hypertensive patients. Depending on the treatment, Klebsiella oxytoca, Klebsiella pneumoniae and Enterobacter sakazakii isolates showed higher multidrug resistance rates in hypertensive patients who have undergone antihypertensive treatment than those without antihypertensive treatment. These results show that antihypertensive drugs expose hypertensive patients to multidrug-resistant bacteria7.
Coinfection is the simultaneous infection of a host by multiple pathogen species. This study shows that Proteus-Klebsiella spp., co-infection was the most frequent in the study population. The high frequency of this co-infection is explained by the fact that Proteus and Klebsiella spp., are the most representative genera colonizing the lower intestinal tract of humans27. The study also shows that Enterobacter-Klebsiella spp., co-infection and Enterobacter.-Klebsiella spp., co-infections were only observed in hypertensive patients. This result proves that hypertensive patients are more exposed to bacterial infections than non-hypertensive patients. This could be explained by the lowering of the immune system because of dysbiosis or certain antihypertensive drugs taken by hypertensive patients7. The above findings are of great importance for public health, as the antibiotic resistance of pathogenic enterobacteria in patients with hypertension and the contribution of treatment to the resistance of these bacteria, have not been systematically researched in patients with hypertension. The results of this study would certainly contribute to the awareness and prevention of multidrug-resistant enteric infections in people with hypertension. Two main limitations could be considered. Firstly, the cross-sectional study design limits the ability to address causal relationships between bacterial resistance and hypertension. Secondly, a study with a larger population size would be required to bring out the relationship between antihypertensive use and bacterial resistance.
CONCLUSION
The study showed that Enterobacter cloacae, Klebsiella oxytoca, Klebsiella pneumoniae, Salmonella typhi and Proteus mirabilis isolates were the most frequent bacteria in hypertensive patients. All bacterial isolates were more frequent in hypertensive patients who had undergone antihypertensive treatment than those without antihypertensive treatment. The multidrug resistance of Klebsiella pneumoniae and Klebsiella oxytoca was significantly higher in hypertensive patients than non-hypertensive patients. The study also revealed an association between antibiotic resistance and hypertension. The results underline the need for the prevention and management of enteric infections in patients with hypertension at the Laquintinie Hospital in Douala.
SIGNIFICANCE STATEMENT
This study aimed to determine the relationship between the resistance profile of pathogenic enterobacteria, hypertension and its treatment. It showed that K. oxytoca, K. pneumoniae and E. sakazakii isolates showed the highest multidrug resistance rates in hypertensive patients undergoing antihypertensive treatment. A strong association between hypertension and bacterial resistance has been found. This study allows us to conclude that hypertensive patients undergoing antihypertensive treatment are susceptible to multi-resistant bacterial infections. These results encourage us to further explore the link between hypertension and antibiotic resistance, by determining the virulence and resistance factors that would explain the high rate of bacterial resistance in hypertensive patients.
REFERENCES
- Hall, J.E., J.M. do Carmo, A.A. da Silva, Z. Wang and M.E. Hall, 2015. Obesity-induced hypertension: Interaction of neurohumoral and renal mechanisms. Circ. Res., 116: 991-1006.
- Lawoyin, T.O., M.C. Asuzu, J. Kaufman, C. Rotimi, E. Owoaje, L. Johnson and R. Cooper, 2002. Prevalence of cardiovascular risk factors in an African, Urban inner city community. West Afr. J. Med., 21: 208-211.
- Cai, M., L. Lin, F. Jiang, Y. Peng, S. Li, L. Chen and Y. Lin, 2023. Gut microbiota changes in patients with hypertension: A systematic review and meta-analysis. J. Clin. Hypertens., 25: 1053-1068.
- Yang, Z., Q. Wang, Y. Liu, L. Wang and Z. Ge et al., 2023. Gut microbiota and hypertension: Association, mechanisms and treatment. Clin. Exp. Hypertens., 45.
- Li, Y., R. Fu, R. Li, J. Zeng, T. Liu, X. Li and W. Jiang, 2023. Causality of gut microbiome and hypertension: A bidirectional mendelian randomization study. Front. Cardiovasc. Med., 10.
- Kamada, N., S.U. Seo, G.Y. Chen and G. Núñez, 2013. Role of the gut microbiota in immunity and inflammatory disease. Nat. Rev. Immunol., 13: 321-335.
- Cao, D.Y., J.F. Giani, L.C. Veiras, E.A. Bernstein and D. Okwan-Duodu et al., 2021. An ACE inhibitor reduces bactericidal activity of human neutrophils in vitro and impairs mouse neutrophil activity in vivo. Sci. Transl. Med., 13.
- Odetoyin, B.W., O. Olaniran, D.O. Afolayan, I.A. Aderibigbe, O. Alaka and A.A. Onanuga, 2018. Asymptomatic bacteriuria in an apparently healthy population and its relation to hypertension. Afr. J. Clin. Exp. Microbiol., 19: 282-290.
- Magiorakos, A.P., A. Srinivasan, R.B. Carey, Y. Carmeli and M.E. Falagas et al., 2012. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect., 18: 268-281.
- Fongang, H., A.T. Mbaveng and V. Kuete, 2023. Global Burden of Bacterial Infections and Drug Resistance. In: African Flora to Fight Bacterial Resistance, Part I: Standards for the Activity of Plant-Derived Products, Kuete, V. (Ed.), Academic Press, Cambridge, Massachusetts, ISBN: 9780443158162, pp: 1-20.
- Weinstein, M.P. and J.S. Lewis II, 2020. The clinical and laboratory standards institute subcommittee on antimicrobial susceptibility testing: Background, organization, functions, and processes. J. Clin. Microbiol., 58.
- Ngalani, O.J.T., A.T. Mbaveng, W.J.T. Marbou, R.Y. Ngai and V. Kuete, 2019. Antibiotic resistance of enteric bacteria in HIV-infected patients at the Banka Ad-Lucem Hospital, West Region of Cameroon. Can. J. Infect. Dis. Med. Microbiol., 2019.
- Princewel, F., S.N. Cumber, J.A. Kimbi, C.N. Nkfusai and E.I. Keka et al., 2019. Prevalence and risk factors associated with hypertension among adults in a rural setting: The case of Ombe, Cameroon. Pan Afr. Med. J., 34.
- Tesfaye, F., P. Byass and S. Wall, 2009. Population based prevalence of high blood pressure among adults in Addis Ababa: Uncovering a silent epidemic. BMC Cardiovasc. Disord., 9.
- Choi, H.M., H.C. Kim and D.R. Kang, 2017. Sex differences in hypertension prevalence and control: Analysis of the 2010-2014 Korea National Health and Nutrition Examination Survey. PLoS ONE, 12.
- Liu, B., H. Liu, R. Na, X. Li and Q. Li et al., 2019. A comparison on prevalence of hypertension and related risk factors between island and rural residents of Dalian City, China. Int. J. Hypertens., 2019.
- Asemu, M.M., A.W. Yalew, N.D. Kabeta and D. Mekonnen, 2021. Prevalence and risk factors of hypertension among adults: A community based study in Addis Ababa, Ethiopia. PLoS ONE, 16.
- Dzotam, J.K. and V. Kuete, 2017. Antibacterial and antibiotic-modifying activity of methanol extracts from six Cameroonian food plants against multidrug-resistant enteric bacteria. BioMed Res. Int., 2017.
- Kuete, V., J.D. Wansi, A.T. Mbaveng, M.M.K. Sop and A.T. Tadjong et al., 2008. Antimicrobial activity of the methanolic extract and compounds from Teclea afzelii (Rutaceae). South Afr. J. Bot., 74: 572-576.
- Seukep, J.A., L.P. Sandjo, B.T. Ngadjui and V. Kuete, 2016. Antibacterial and antibiotic-resistance modifying activity of the extracts and compounds from Nauclea pobeguinii against Gram-negative multi-drug resistant phenotypes. BMC Complementary Altern. Med., 16.
- Itah, A.Y. and A.E. Ben, 2004. Incidence of enteric bacteria and Staphylococcus aureus in day care centers in Akwa Ibom State, Nigeria. Southeast Asian J. Trop. Med. Public Health, 35: 202-209.
- Mouiche, M.M.M., F. Moffo, J.F.T.K. Akoachere, N.H. Okah-Nnane and N.P. Mapiefou et al., 2019. Antimicrobial resistance from a one health perspective in Cameroon: A systematic review and meta-analysis. BMC Public Health, 19.
- Duytschaever, G., G. Huys, L. Boulanger, K. de Boeck and P. Vandamme, 2013. Amoxicillin-clavulanic acid resistance in fecal Enterobacteriaceae from patients with cystic fibrosis and healthy siblings. J. Cystic Fibrosis 12: 780-783.
- Gould, K., 2016. Antibiotics: From prehistory to the present day. J. Antimicrob. Chemother., 71: 572-575.
- Biliński, J., P. Grzesiowski, J. Muszyński, M. Wróblewska and K. Mądry et al., 2016. Fecal microbiota transplantation inhibits multidrug-resistant gut pathogens: Preliminary report performed in an immunocompromised host. Arch. Immunol. Ther. Exp., 64: 255-258.
- Kengne, M.F., O.D. Tsobeng, B.S.T. Dadjo, V. Kuete and A.T. Mbaveng, 2024. Multidrug resistant enteric bacteria from cancer patients admitted in Douala Laquintinie Hospital, Littoral Region of Cameroon. Can. J. Infect. Dis. Med. Microbiol., 2024.
- Drzewiecka, D., 2016. Significance and roles of Proteus spp. bacteria in natural environments. Microb. Ecol., 72: 741-758
How to Cite this paper?
APA-7 Style
Tsobeng,
O.D., Kengne,
M.F., Dadjo,
B.S., Kuete,
V. (2025). Multidrug Resistance of Bacteria Causing Enteric Infections in Patients with Arterial Hypertension at the Douala Laquintinie Hospital in Cameroon. Asian Journal of Biological Sciences, 18(2), 263-274. https://doi.org/10.3923/ajbs.2025.263.274
ACS Style
Tsobeng,
O.D.; Kengne,
M.F.; Dadjo,
B.S.; Kuete,
V. Multidrug Resistance of Bacteria Causing Enteric Infections in Patients with Arterial Hypertension at the Douala Laquintinie Hospital in Cameroon. Asian J. Biol. Sci 2025, 18, 263-274. https://doi.org/10.3923/ajbs.2025.263.274
AMA Style
Tsobeng
OD, Kengne
MF, Dadjo
BS, Kuete
V. Multidrug Resistance of Bacteria Causing Enteric Infections in Patients with Arterial Hypertension at the Douala Laquintinie Hospital in Cameroon. Asian Journal of Biological Sciences. 2025; 18(2): 263-274. https://doi.org/10.3923/ajbs.2025.263.274
Chicago/Turabian Style
Tsobeng, Ornella, Djiolieu, Michael Francis Kengne, Ballue Serges Tatiefo Dadjo, and Victor Kuete.
2025. "Multidrug Resistance of Bacteria Causing Enteric Infections in Patients with Arterial Hypertension at the Douala Laquintinie Hospital in Cameroon" Asian Journal of Biological Sciences 18, no. 2: 263-274. https://doi.org/10.3923/ajbs.2025.263.274

This work is licensed under a Creative Commons Attribution 4.0 International License.