Prevalence of Hepatitis B and Hepatitis C Among the Abroad Job Seekers in a Selective Diagnostic Centre of Chattogram, Bangladesh
-
Noman P. Chowdhury
Department of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram 4202, Bangladesh
Md.E. IslamDepartment of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram 4202, Bangladesh
Sadia RaihanDepartment of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram 4202, Bangladesh
Gazi W. Akbar

Department of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram 4202, Bangladesh
Nurul AbsarDepartment of Biochemistry and Biotechnology, University of Science and Technology Chittagong, Chattogram 4202, Bangladesh
Background and Objective: Hepatitis B and C pose major global public health challenges, especially among migrant populations, including job seekers pursuing overseas employment. These individuals are often at increased risk due to limited access to healthcare and inadequate disease awareness. This study aimed to assess the prevalence of hepatitis B and C among individuals seeking foreign employment at a selective diagnostic center in Chattogram, Bangladesh. Materials and Methods: A cross-sectional study was conducted involving 726 individuals (aged 18-57 years) undergoing medical screening for overseas employment, primarily to the Middle East. Participants were selected from the Chattogram Division, including those intending to work abroad and returnee migrant workers. Data were collected using a structured questionnaire, and blood samples were tested for Hepatitis B Surface Antigen (HBsAg) and anti-HCV antibodies. Descriptive statistics and Chi-square tests were used for data analysis (p<0.05). Results: Of the 726 participants, 93.11% (n = 676) were male and 6.89% (n = 50) were female. A total of 4.3% (n = 31) tested positive for hepatitis: 3.44% (n = 25) were HBsAg-positive and 0.82% (n = 6) were anti-HCV-positive. The highest prevalence was observed in individuals from the Chattogram and Cumilla districts. Education level was significantly associated with awareness and knowledge of hepatitis (p<0.05). Conclusion: The study highlights a measurable prevalence of hepatitis B and C among job seekers from Chattogram, suggesting their heightened vulnerability due to poor awareness and limited healthcare access. Broader, nationwide screening and education programs, including molecular diagnostic approaches, are essential for early detection and prevention in this at-risk population.
| Copyright © 2025 Chowdhury et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Globally, viral hepatitis caused by the hepatitis B and C viruses is a serious public health concern. For hundreds of millions of individuals, the hepatitis B and C virus causes chronic conditions1. Hepatitis B is a vaccine-preventable liver infection caused by the Hepatitis B Virus (HBV)2.
When an infected person’s blood, semen, or other bodily fluids get into an uninfected person’s body, they can spread hepatitis B. Possible effects include sharing syringes, needles, or other injectable supplies, having sex, or becoming pregnant or giving birth2. Although not all newly infected individuals develop symptoms, those who do may experience jaundice, nausea, stomach pain, lethargy, and low appetite. Many people have hepatitis B for only a short amount of time. Others may develop a chronic, long-lasting infection that can result in major, perhaps fatal conditions, including liver disease or liver cancer. The likelihood that hepatitis B will become chronic depends on age3. A person’s risk of acquiring a chronic infection increases with their age at hepatitis B virus infection. Approximately 9 to 10 newborns who develop an infection go on to develop a chronic, lifelong infection2. As a child grows older, the risk reduces. One in three children who have hepatitis B before the age of 6 will eventually go on to develop chronic hepatitis B. In contrast, nearly all adults and children aged 6 and up who encounter the hepatitis B virus fully recover and do not experience chronic infection4. Vaccination is the most effective method of preventing hepatitis B. The vaccination should be administered to all adults between the ages of 18 and 59, and it can be administered to any adult who asks it5. Screening should be done at least once in a lifetime for all persons who are 18 years of age or older.
The hepatitis C virus causes hepatitis C, which is an inflammation of the liver. The virus can cause acute or chronic hepatitis, which can range in severity from a small illness to a serious, lifelong condition that includes liver cirrhosis and cancer. The majority of hepatitis C infections are brought on by blood exposure from unsafe injection practices, risky medical treatments, unscreened blood transfusions, injectable drug use, and sexual behaviours that expose people to blood6. Over 1.5 million new cases of hepatitis C virus infection are reported each year, and an estimated 58 million people worldwide are infected with the virus chronically. A chronic hepatitis C infection affects an estimated 3.2 million youth. Antiviral drugs can cure over 95% of hepatitis C patients, but diagnosis and therapy are not commonly accessible. There isn’t an effective hepatitis C vaccination available right now7.
Antiviral drugs can be used to treat hepatitis B and C, which can both be identified by blood testing. There is no vaccination to prevent hepatitis C, although there are vaccines to prevent hepatitis B. Avoiding exchanging needles or other drug supplies, practicing safe sex, and being tested for HBV and HCV in case you feel you may be at risk are all crucial. Serious liver damage and associated complications can be avoided or lessened with early detection and treatment of viral hepatitis5,7.
The prevalence of HBV infections varies by country and is closely linked to environmental and behavioural factors. The prevalence of HBV infection is “intermediate”, ranging from 2 to 7%, over the Indian Subcontinent, which includes Bangladesh, Central Asia, and South America. Of cases of chronic hepatitis, HBV accounts for 76.3%, whereas HCV causes 24.1%. The frequency of the hepatitis B virus in Bangladesh is 7.8% among foreign job seekers and 4.9-6.25% among the general population. The general population and the highest-risk demographics have an HCV infection prevalence of 1 to 2.2%8.
One of the main countries from which migrant laborers come is Bangladesh. Approximately 500,000 Bangladeshis leave the country each year to work overseas. Through remittances, migrant workers collectively contribute between 7 and 8% of the nation’s GDP, supporting its development and advancement. The countries that hire the most Bangladeshi workers are Oman and Saudi Arabia, with Qatar following in second (BMET 2016). The majority of male migrant workers are hired for construction jobs, whereas the majority of female migrant workers are hired for domestic maid services. Bangladeshi migrants frequently migrate in unsafe circumstances, which raises their risk of developing HBV and HCV infections, despite the significant economic gains they produce from employment in the Gulf.
The main purpose of this study was to investigate the prevalence of hepatitis B and C in job seekers looking for work overseas. It also includes other objectives, such as:
| • | To understand the socio-demographic characteristics of the respondents | |
| • | To determine which age group is mostly affected | |
| • | To determine the risk factors related to Hepatitis B and C | |
| • | To know the knowledge of Hepatitis B and C among job seekers abroad |
MATERIALS AND METHODS
Study area: A descriptive cross-sectional study was conducted to determine the prevalence of Hepatitis B and Hepatitis C among international job seekers. This study was carried out in the diagnostic laboratory of Chattogram city for medical screening, which is authorized by the Gulf Approved Medical Centers Association (GAMCA). A total of 726 healthy adults who intend to go abroad, mainly Middle East, for different job purposes, and the immigrant workers already worked in different countries were analyzed in this study. The study was conducted during the months of January, 2021 to June, 2021.
Sample collection: The inclusion criteria for this study include immigrant workers above 18 years old referred by the Gulf Approved Medical Centers Association (GAMCA) authority, and no exclusion criteria were referred by the GAMCA authority.
Data collection procedure: During the data collection period for accumulating data from the participants and fulfilling the aim and objectives of the study, the patients had to fill out a consent form Appendix 1.
A pre-tested structured interview schedule was used to collect information on selected sociodemographic characteristics, history of jaundice, receipt of blood transfusion, and use of parenteral injections. The questionnaire (Appendix 2) was administered before blood sample collection by the investigator and trained technicians who had been previously oriented with the instrument. Each respondent’s blood sample was labeled with a unique code number, which was duly recorded.
The ELISA Method was used to measure HBsAg and HCV. Enzyme immunoassay was used to check each serum sample for HBV and HBsAg (Bio-Rad, USA). Every laboratory test was conducted by the guidelines provided by the manufacturers. Finally, HBsAg was given a questionnaire and immigrants with HCV. The purpose of the questions was to gauge their understanding of HBsAg and HCV symptoms, contributing causes, preventative strategies, etc.
| Appendix 1: | Informed consent form | |||
| I am Mr./Mrs ________________________________ hereby giving inform consent willingly to participate in the study to be conducted by Md. Noman Parvez Chowdhury without any prejudice. I am fully convinced that during study, I will not suffer from any serious physical or psychological problems. I am also informed that my participation will bring fruitful results that will be beneficial for health issues. I have the right to withdraw from this study at any time. I will not receive any financial benefit. I have understood that the personal information will be kept strictly confidential and will be used for research purpose only. |
| ________________________________________________ |
| Signature/Thumb impression of respondents |
| Date: ____________________________________________________________________ |
| Name: __________________________________________________________________ |
Address: ________________________________________________________________ |
| Signature of witness: __________________________________________________ |
| Signature of the investigator: _________________________________________ |
| Appendix 2: | Questionnaire | |||
 |
||||||
| SL No: ___________________________ | Date: ___________________________ | |||||
| Title: Prevalence of hepatitis B and C among the abroad job seekers | ||||||
| (A) | GENERAL INFORMATION | |||||
| 1 | Name of the respondent: ________________________________________________________________________________________________________ | |||||
| 2 | Address: __________________________________________________________________________________________________________________________ | |||||
| Village: ___________________________________________________________ P.O: _______________________________________________________________ | ||||||
| Upazila: __________________________________________________________ District: ___________________________________________________________ | ||||||
| 3 | Age _______________________ years | |||||
| 4 | Gender: | |||||
| (a) Male | (b) Female | (c) Others | ||||
| 5 | Religion: | |||||
| (a) Islam | (b) Hinduism | (c) Buddhism | (d) Christianity | (e) Others | ||
| 6 | Marital Status: | |||||
| (a) Married | (b) Unmarried | (c) Widowed | (d) Others | |||
| 7 | Educational Status: | |||||
| (a) Primary/equivalent | (b) Secondary/equivalent | (c) HSC/equivalent | (d) Graduate and above | |||
| 8 | Occupation: | |||||
| (a) Unemployment | (b) Service holder | (c) Student | ||||
| (d) Businessman | (e) Cultivation | (f) Other | ||||
| 9 | Socio-economic status: | |||||
| Monthly income (TK.) | Score | Housing condition | Score | |||
| <3,000 | 1 | 1 | ||||
| 3,000-5,000 | 2 | 2 | ||||
| 5,000-10,000 | 3 | 3 | ||||
| >10,000 | 4 | |||||
| Housing condition | Score | |||||
| Asset | Score | 1 | ||||
| None | 1 | 2 | ||||
| Simple belongings | 2 | 3 | ||||
| Cultivable land | 3 | |||||
| <5 bighas | 4 | |||||
| SES ________________ Score | ||||||
| (a) Lower class (2-4) | (b) Upper middle class (8-10) | |||||
| (c) Lower middle class (5-7) | (d) Upper class (>10) | |||||
| 10 | What kind of family do you live in? | |||||
| (a) Joint | (b) Nuclear | (c) Extended | ||||
| 11 | Numbers of family members? | |||||
| (a) 1-3 | (b) 4-5 | (c) >6 | ||||
| (B) | SPECIFIC INFORMATION | |||||
| 1 | Have you immigrated before? | |||||
| (a) Yes | (b) No | |||||
| 2 | Which country did you immigrate to before? | |||||
| (a) Dubai | (b) Oman | (c) Saudi Arabia | ||||
| (d) Qatar | (e) Kuwait | (f) Bahrain | ||||
| 3 | How long have you stayed in the immigrant country? | |||||
| (a) 1-2 years | (b) 3-4 years | (c) >5 years | ||||
| 4 | What types of work did you do in the immigrant country? | |||||
| (a) Labour | (b) Driver | (c) Salesman | (d) Other | |||
| 5 | Have you heard about Hepatitis? | |||||
| (a) Yes | (b) No | |||||
| 6 | Do you have any symptoms? | |||||
| (a) Yes | (b) No | |||||
| 7 | Do any of your relatives or friends have Hepatitis? | |||||
| (a) Yes | (b) No | |||||
| 8 | Have you ever been tested for Hepatitis before? | |||||
| (a) Yes | (b) No | |||||
| 9 | Are there any ways to protect yourself against Hepatitis? | |||||
| (a) Yes | (b) No | |||||
| 10 | Any other information: | _________________________________________________________________________________________________________ | ||||
| Thanks for your cordial cooperation. | ||||||
| Data Collector | ||||||
| Name: __________________________________________ | ||||||
| ID: ______________________________________________ | ||||||
Data analysis: The data analysis was performed in the Statistical Package for Social Science (SPSS) version 26.0 (SPSS Inc., Chicago, Illinois, USA) and Microsoft Excel 2010. Each study subject had been given a code number, and each question was accounted as a variable. Each variable of the questionnaire is defined in the means of variable name, type, width, decimals, label, values, missing, column, align, and measure in the variable view of SPSS spreadsheet and Microsoft Excel 2010. The code numbers of subjects and variables are labeled in the list of values in the variable view. Finally, the computerized data was prepared for analysis. The prevalence of hepatitis B and C among the abroad job seekers last 2 months was calculated using frequencies and percentages.
RESULTS
In this study, a total of 726 immigrant workers (100%) participated. All participants were over the age of 18 and were referred by the Gulf Approved Medical Centers Association (GAMCA) to seek employment primarily in the Middle East, with many having previously worked in various countries. Data collection occurred from January, 2021 to June, 2021. The demographic analysis revealed that 93.11% (n = 676) of the participants were male, while 6.89% (n = 50) were female. The findings and observations are displayed in Table 1. The p-value obtained is extremely small (<0.05), and the difference in gender distribution is statistically significant. This means the observed distribution (93.11% male, 6.89% female) deviates significantly from an equal gender distribution, and this deviation is not due to random chance.
| Table 1: | Distribution of the respondents according to gender | |||
| Gender | Number | Percentage (%) | χ2 | p-value |
| Male in number (n) | 676 | 93.11 | 539.77 | 2.11×1011 |
| Female in number (n) | 50 | 6.89 | ||
| Total respondents | 726 | 100 |
| Table 2: | Percentage of male and female among the HBsAg and HCV positive | |||
| Title | Numbers | Percentage (%) |
| Male numbers (n) | 29 | 93.5 |
| Female numbers (n) | 2 | 6.5 |
| Positive respondents | 31 | 100 |
| Table 3: | Prevalence of HBsAg and HCV infection in apparently healthy adults of different genders | |||
| Gender | Number | HBV positive case |
HBV infection prevalence rate (%) |
HCV positive case |
HCV infection prevalence rate (%) |
| Male | 676 | 23 | 3.4 | 6 | 0.8 |
| Female | 50 | 2 | 4 | 0 | 0 |
| Total respondents | 726 | 25 | 3.44 | 6 | 0.82 |
| Table 4: | Distribution of respondents according to age | |||
| Age group | Number | HBV positive case |
HBV infection prevalence rate (%) |
HCV positive case |
HCV infection prevalence rate (%) |
| 18-28 | 367 | 12 | 3.2 | 3 | 0.81 |
| 29-38 | 265 | 10 | 3.2 | 2 | 0.75 |
| 39-48 | 75 | 2 | 2.6 | 1 | 1.1 |
| >49 | 19 | 1 | 5.2 | 0 | 0 |
| Total | 726 | 25 | 3.44 | 6 | 0.82 |
As shown in Table 2, of the 726 immigrants, 4.3% (n = 31) tested positive for HBsAg and HCV, while 95.7% (n = 695) were negative. It was discovered that out of thirty-one (n = 31) HBsAg and HCV positive immigrants, 29 (n = 29) were male and 2 (n = 2) were female. Males outnumbered females. A Chi-square value of 0 with p = 1 typically indicates that the observed distribution matches the expected distribution perfectly or sample sizes (especially for positive cases) are too small for meaningful differentiation. Again, as depicted in Table 3. Among the 726 immigrants, 3.44% (n = 25) were found HBsAg positive and 0.82% (n = 6) were found HCV positive. However, statistical analysis revealed no significant association between gender and infection status for either HBV or HCV (p>0.05).
From the questionnaire (Appendix 2), the age of participants was recorded and represented in Table 4, as shown in the table it was found that respondents in the 18-28 age range had the highest number of infections (n = 12), followed by those in the 29-38 age range (n = 10). Only 1 participant was found in the >49 age group, while the 39-48 age group had 2 participants. It was observed in HCV that the 18-28 age group (n = 03) was more at risk than any other age group. The 29-38 age group had the second highest number of infections (n = 02). The 39-48 age group only had one infected person, and the age groups over 49 had no infected participants. The p-values for both HBV and HCV are much greater than 0.05. This indicates that there is no statistically significant association between age group and infection status (for either HBV or HCV) at the 5% significance level.
Table 5 showed that individuals with primary education had the highest number of infections (n = 16), followed by those with secondary education (n = 14), and only one person (n = 01) with higher secondary or diploma education was infected. However, statistical analysis (Chi-square test) revealed no significant association between educational status and infection prevalence for HBV or HCV.
| Table 5: | Distribution of respondents according to educational status | |||
| Educational status | Number | HBV positive case |
HBV infection prevalence rate (%) |
HCV positive case |
HCV infection prevalence rate (%) |
| Primary | 341 | 13 | 3.81 | 3 | 0.87 |
| Secondary | 360 | 11 | 3.05 | 3 | 0.83 |
| Higher secondary/diploma | 25 | 1 | 4 | 0 | 0 |
| Total | 726 | 25 | 3.44 | 6 | 0.82 |
| Table 6: | Distribution of respondents according to occupation | |||
| Title | Number | HBV positive case |
HBV infection prevalence rate (%) |
HCV positive case |
HCV infection prevalence rate (%) |
| Unemployed | 63 | 3 | 4.7 | 0 | 0 |
| Cultivation | 151 | 5 | 3.3 | 1 | 0.6 |
| Student | 39 | 1 | 2.5 | 0 | 0 |
| Service | 135 | 4 | 2.9 | 1 | 0.7 |
| Business | 59 | 2 | 3.3 | 0 | 0 |
| Others | 279 | 10 | 4.3 | 4 | 1.4 |
| Total | 726 | 25 | 3.44 | 6 | 0.82 |
| Table 7: | Socio-demographic characteristics of the respondents (n = 31) | |||
| Variables | Frequency (n) | Percentage (%) |
| Age | ||
| 18-28 | 15 | 48.4 |
| 29-38 | 12 | 38.7 |
| 39-48 | 3 | 9.7 |
| >49 | 1 | 3.2 |
| Gender | ||
| Male | 29 | 94 |
| Female | 2 | 6 |
| Total | 31 | 100 |
| Education level | ||
| Primary | 16 | 51.6 |
| Secondary | 14 | 45.2 |
| Higher secondary/diploma | 1 | 3.2 |
| Graduate | 0 | 0 |
| Total | 31 | 100 |
| Professional | ||
| Unemployed | 3 | 9.7 |
| Cultivation | 6 | 19.4 |
| Student | 1 | 3.2 |
| Service | 5 | 16.1 |
| Business | 2 | 6.4 |
| Others (homemaker, driver, salesman) | 14 | 45.2 |
| Total | 31 | 100 |
From the data observed in Table 6, n = 63 of the respondents were unemployed, n = 151 were engaged in agricultural work, n = 39 were students, n = 135 were employed in various services, n = 59 owned their businesses, and n = 279 held other jobs such as driving, cleaning, plumbing, construction, housekeeping, and so on. These results suggest that within this sample of 726 respondents, no statistically significant association was found between occupation and infection status (p>0.05 for both).
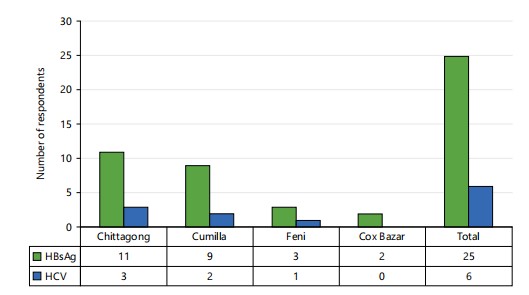
As per the record from the questionnaire (Appendix 2), the highest prevalence of disease among immigrants is found in the Chattogram district, with HBsAg (n = 11) and HCV (n = 3). Cumilla has HBsAg (n = 9) and HCV (n = 2). Feni has HBsAg (n = 3) and HCV (n = 1), and Cox Bazar has HBsAg (n = 2), but no HCV, as shown in Fig. 1. However, statistical analysis revealed no significant association between district and type of infection, indicating a relatively even distribution of viral hepatitis cases across the districts (p>0.05).
|
|
In the study, a formatted questionnaire (Appendix 2) was used as a data collection tool. Interviews were held with clinically confirmed hepatitis-positive participants. All the respondents who tested positive for hepatitis were over 18 years old, including two (n = 2) females and twenty-nine (n = 29) males. Among the 31 respondents who tested positive for hepatitis, 16 (n = 16) had a primary school education, 14 (n = 14) had a secondary school education, and just one (n = 1) had a higher secondary school diploma or diploma, as shown in Table 7. Again, the p>0.05 indicates no statistically significant association between education level and type of profession (formal vs informal) in this group of respondents. Most were aged between 18-28 years (48.4%) and male (93.5%). Regarding education, the majority had a primary education (51.6%), and in terms of occupation, a significant portion were involved in various other jobs such as driving, homemaking, or sales (45.2%).
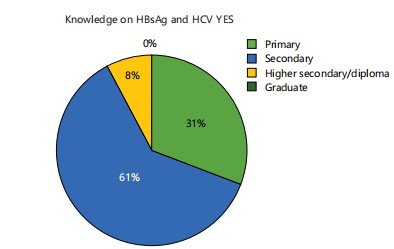
This study found that out of 31 positive immigrants, 16 had received primary education, 14 had completed secondary education, and only one had earned a higher secondary or diploma degree. Four of the sixteen primary-educated immigrants knew HCV and HBsAg, while the majority of secondary-educated immigrants (n = 14) knew HCV and HBsAg. Immigrants with higher secondary education or diplomas knew HCV and HBsAg, as shown in Fig. 2.
DISCUSSION
Many demographic and socioeconomic factors have a major impact on the dynamics of viral hepatitis in Bangladesh. Comprehensive prevalence surveys are frequently impractical due to financial limitations, which makes focused research among certain populations, like the 726 migrant workers in this study. The total prevalence of HBsAg and HCV among these subjects was 4.26% (93.11% male; 6.89% female), which is in close agreement with the ~3.1-5.5% national HBsAg prevalence7. Chattogram reported the highest number of positive cases, possibly due to its densely populated migrant communities. This is in line with previous studies that found geographic clusters of hepatitis B in urban areas with high migrant inflows8.
The frequency of HBsAg was 3.44% (male 92%, female 8%), and the prevalence of HCV was 0.82%, with all HCV cases occurring in males, as shown in Table 1. These numbers are in good agreement with estimates of the general and immigrant populations (HCV 0.2-1%)-a pattern consistent with earlier research identifying geographical clusters of hepatitis B in urban areas with dense migrant inflows similar HCV prevalence (0.09-0.6%) have also been reported among immigrants from Bangladesh living in Europe9. In contrast, the HCV prevalence of 0.82% exclusively among male respondents is in good agreement with previously reported ranges for both the general Bangladeshi population and expatriates living in Europe (0.2-1%)10. The prevalence is less than 1% in the general population; however, greater rates are observed in high-risk populations such as intravenous drug users (up to 24.8%)9.
The results of both international and regional investigations were supported by a statistically significant connection (p<0.031) found between education level and hepatitis awareness. School-based interventions show that education significantly enhances awareness, attitudes, and preventive practices about HBV and HCV, reported by Kaushal et al.11. Education is an essential way of spreading health messages, especially to people of reproductive age (18-38 years), who may be more susceptible to transmission if they lack the necessary information and resources. Similarly, a research by Bhogal et al.12 highlighted the importance of focused health education programs in increasing reproductive-age individuals’ understanding about hepatitis, particularly among those in underserved or migrant areas.
Overall, our research emphasizes the significance of individualized instruction and focused screening for lower-middle-class and male-dominated immigrant groups. These results support the body of research showing that, in environments with limited resources, raising sociodemographic characteristics especially education can raise hepatitis awareness and, eventually, lower the disease burden.
Despite these insights, this study has a number of limitations. It was only carried out at a diagnostic facility in Chattogram City that has pre-departure medical screening authorisation from the Gulf Approved Medical Centres Association (GAMCA). Due to this, the results could not accurately represent the state of the country as a whole. In addition, the study cohort was made up of people who were screened and appeared to be in good health, which would have resulted in an underestimation of the true prevalence, especially among carriers who showed no symptoms.
Furthermore, there was a notable gender imbalance, with far more men than women participating, which limited the applicability of findings based on gender. Also, there aren’t many similar studies that concentrate exclusively on Bangladeshi immigrant communities, which limits the capacity to compare results in a larger migratory environment. Additionally, important factors such as virus genotypes, risk behaviour profiles, and hepatitis vaccination status were not evaluated. Future research should address these limitations by aiming for fair demographic representation, greater geographic sampling, and the inclusion of molecular diagnostics in order to provide a more thorough understanding of the dynamics of hepatitis transmission.
CONCLUSION
Viral hepatitis can cause serious long-term health issues, including liver disease and cancer. Although this study focused on a specific group mostly healthy, low-income male immigrants it offers valuable insights into hepatitis risks among migrant workers in Bangladesh. The findings highlight poor access to health education and care, along with systemic issues in the migration process. While hepatitis B rates appear to be declining and hepatitis C remains low, larger and more comprehensive studies are needed to accurately assess national prevalence and guide public health strategies.
ETHICAL CONSIDERATION
Institutional consent was obtained from the Institutional Ethics Committee of the Turkey Medical Services (TMS), Chattogram. The results were included to keep them confidential and strictly for academic purposes. Clinical specimens were assigned specific identification numbers to maintain their anonymity.
SIGNIFICANCE STATEMENT
In Bangladesh, viral hepatitis is still a serious public health issue, especially for nomadic and socioeconomically disadvantaged groups. However, resource limitations limit the availability of complete national-level data. By assessing the prevalence and knowledge of Hepatitis B (HBsAg) and Hepatitis C (HCV) among 726 migrant workers undergoing required health screening in Chattogram, this study fills that knowledge gap. The results showed a statistically significant correlation between education level and hepatitis awareness (p<0.031) and a combined hepatitis prevalence of 4.26%, with higher rates among males. These findings highlight the importance of education in preventing disease and are consistent with national prevalence estimates. This study’s wider significance stems from its capacity to guide focused public health initiatives, particularly education-based awareness campaigns, among vulnerable, low-income, and immigrant populations.
REFERENCES
- Adegbamigbe, O.J., M. Yusuf, K.A. Durowade, O.O. Oguntoye and Y. Ogundare, 2022. Exposure to patients' sample and prevalence of hepatitis B and C virus infection among health-care workers in a Nigerian tertiary hospital. Ann. Afr. Med., 21: 322-326.
- Kamani, L., 2025. Viral Hepatitis in Pregnancy. In: Hepatology: An Evidence-Based Clinical Compendium, Satapathy, S.K., Mamun-Al-Mahtab and S.P. Singh (Eds.), Elsevier, Amsterdam, Netherlands, ISBN: 978-0-443-30052-3, pp: 971-1001.
- Hyams, K.C., 1995. Risks of chronicity following acute hepatitis B virus infection: A review. Clin. Infect. Dis., 20: 992-1000.
- Lok, A.S.F. and B.J. McMahon, 2009. Chronic hepatitis B: Update 2009. Hepatology, 50: 661-662.
- Weng, M.K., M. Doshani, M.A. Khan, S. Frey and K. Ault et al., 2022. Universal hepatitis B vaccination in adults aged 19-59 years: Updated recommendations of the advisory committee on immunization practices-United States, 2022. Morbidity Mortality Wkly Rep., 71: 477-483.
- Feld, J.J. and J.H. Hoofnagle, 2005. Mechanism of action of interferon and ribavirin in treatment of hepatitis C. Nature, 436: 967-972.
- Manns, M.P. and B. Maasoumy, 2022. Breakthroughs in hepatitis C research: From discovery to cure. Nat. Rev. Gastroenterol. Hepatol., 19: 533-550.
- Plessz, M., S. Ezdi, G. Airagnes, I. Parizot and C. Ribet et al., 2020. Association between unemployment and the co-occurrence and clustering of common risky health behaviors: Findings from the Constances cohort. PLoS ONE, 15.
- Hassan Uz-Zaman, M., A. Rahman and M. Yasmin, 2018. Epidemiology of hepatitis B virus infection in Bangladesh: Prevalence among general population, risk groups and genotype distribution. Genes, 9.
- Soothill, G., S. Hessey, M. Erotocritou, P. Griffiths and S. Ijaz et al., 2018. Diagnostic utility of hepatitis E virus antigen-specific ELISA versus PCR testing in a cohort of post liver transplant patients in a large university hospital. J. Clin. Virol., 106: 44-48.
- Kaushal, K., P. Aggarwal, N. Dahiya and G. Kumar, 2024. Impact of educational interventions on hepatitis B and C awareness among school students of Delhi NCR, India. BMC Public Health, 24.
- Bhogal, A.S., S. Montagnese and A.R. Mani, 2018. The consideration of heart rate complexity as a co-morbidity factor for liver transplantation selection procedures. Liver Int., 38: 380-380.
How to Cite this paper?
APA-7 Style
Chowdhury,
N.P., Islam,
M.E., Raihan,
S., Akbar,
G.W., Absar,
N. (2025). Prevalence of Hepatitis B and Hepatitis C Among the Abroad Job Seekers in a Selective Diagnostic Centre of Chattogram, Bangladesh. Asian Journal of Biological Sciences, 18(4), 828-838. https://doi.org/10.3923/ajbs.2025.828.838
ACS Style
Chowdhury,
N.P.; Islam,
M.E.; Raihan,
S.; Akbar,
G.W.; Absar,
N. Prevalence of Hepatitis B and Hepatitis C Among the Abroad Job Seekers in a Selective Diagnostic Centre of Chattogram, Bangladesh. Asian J. Biol. Sci 2025, 18, 828-838. https://doi.org/10.3923/ajbs.2025.828.838
AMA Style
Chowdhury
NP, Islam
ME, Raihan
S, Akbar
GW, Absar
N. Prevalence of Hepatitis B and Hepatitis C Among the Abroad Job Seekers in a Selective Diagnostic Centre of Chattogram, Bangladesh. Asian Journal of Biological Sciences. 2025; 18(4): 828-838. https://doi.org/10.3923/ajbs.2025.828.838
Chicago/Turabian Style
Chowdhury, Noman, P., Md. E. Islam, Sadia Raihan, Gazi W. Akbar, and Nurul Absar.
2025. "Prevalence of Hepatitis B and Hepatitis C Among the Abroad Job Seekers in a Selective Diagnostic Centre of Chattogram, Bangladesh" Asian Journal of Biological Sciences 18, no. 4: 828-838. https://doi.org/10.3923/ajbs.2025.828.838

This work is licensed under a Creative Commons Attribution 4.0 International License.